")
")
| Issue |
Radioprotection
Volume 61, Number 2, Avril-Juin 2026
|
|
|---|---|---|
| Page(s) | 126 - 131 | |
| DOI | https://doi.org/10.1051/radiopro/2025028 | |
| Published online | 15 juin 2026 | |
Article
Estimation of entrance surface dose for radiography examinations in Arrazi Hospital from Mohammed VI University Hospital Center of Marrakech (Morocco)
1
Higher Institute of Nursing Professions and Health Technics, Marrakech, Morocco
2
Environmental, Ecological and Agro-Industrial Engineering Laboratory, University Sultan Moulay Sliman, Béni Mellal, Morocco
3
Sultan Moulay Sliman University (LICPM), Faculty of Sciences and Techniques, Department of Physics, B.P.523, 23000 Béni Mellal, Morocco
* Corresponding author: Cette adresse e-mail est protégée contre les robots spammeurs. Vous devez activer le JavaScript pour la visualiser.
Received:
21
December
2024
Accepted:
24
May
2025
Abstract
Diagnostic Reference Levels (DRLs) are an important tool for radiography and radiological science practice optimization. Assessment of entrance surface doses for patients in digital radiography examinations should be made as a means for the optimization of the radiation protection of the patients. This study aims to determine the typical DRLs (TDRL) values based on entrance surface dose (ESD) for routine radiography in Arrazi Hospital at the Mohammed VI University Hospital Centre (ARH Med VI UHC) in Marrakech, Morocco. A total of 1170 radiography examinations (RE) were included. They underwent 13 separate projections in the adult radiology department of the Marrakech-Safi region teaching hospital. The X-ray tube’s dose area product (DAP) was used to figure out the patient’s entrance surface dose for the cervical spine anterior-posterior (AP), cervical spine lateral (LAT), lumbar spine AP/LAT, abdomen AP, pelvis AP, shoulder AP, knee AP/ LAT, skull AP/ LAT, and the chest PA. The TDRL values of ESD for cervical spine AP/LAT, lumbar spine AP/LAT, abdomen AP, pelvis AP, shoulder AP, knee AP/LAT, skull AP/LAT, and chest AP were 1.52 mGy/1.46 mGy, 3.34 mGy/4.76 mGy, 1.56 mGy, 1.98 mGy, 1.25 mGy, 0.58 mGy/0.58 mGy, 2.2 mGy/2.1 mGy, and 0.22 mGy, respectively. We compared our TDRL values with those of other countries. Although the estimated TDRLs are encouraging, significant efforts are needed to reduce them, particularly for shoulder, knee, and skull X-rays.
Key words: Conventional radiology / dose / radiation protection / DAP / ESD / DRL / TDRL
© H. Khajmi et al., Published by EDP Sciences, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
1 Introduction
According to research conducted by the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR, 2000), approximately 4 to 5 billion X-ray examinations are performed worldwide each year. No other imaging technique is utilized on such a large scale. These exams can provide radiologists with efficient diagnostic capabilities for various diseases and at a lower cost. Although the radiation doses from these examinations are generally low and late effects are expected to be minimal, it’s important to ensure that the exposures are justified and optimized in relation to their benefits and risks.
The radiation dose received by a patient during an X-ray examination depends on several factors, including tube current, beam voltage, exposure time, the type of X-ray generator used, and the image receptors. Additionally, the patient dose is significantly affected by technician-specific variables and the procedures employed in radiography. Surveys conducted at national and international levels indicate that the patient dose can vary greatly between different patients and X-ray facilities for the same type of X-ray projection. Therefore, it is crucial to assess the patient dose in any diagnostic X-ray facility (Ciraj et al., 2005; Hart et al., 2009; Roch P. et al., 2013).
To minimize the risks associated with radiation exposure, it is essential to reduce the dose received by patients. This can be achieved through various measures, including quality control of facilities and radiological procedures, as well as the establishment of diagnostic reference levels. The concept of DRLs was introduced by the International Commission on Radiological Protection (ICRP) and the European Commission (EC) (ICRP, 1996; EC, 1999). DRLs were created to promote the optimization of radiation exposure for patients.
Many organizations, including the ICRP (2017), IAEA (2007), and EC (2014), as well as several countries such as Germany (2010), Lithuania (Ziliukas et al., 2010), the UK (Hart et al., 2012), Greece (Metaxas et al., (2019)), France (IRSN 2020), Iran (Mohsenzadeh et al., 2020), and Saudi Arabia (Alrehily, 2022), have been involved in establishing DRLs for diagnostic imaging. In recent years, the concept of DRLs has gained significant interest and importance in Morocco. As a result, several studies have been conducted to determine the DRLs in computed tomography (CT) and in both conventional and interventional radiology (Benmessaoud et al., 2021; El Mansouri et al., 2022; Talbi et al., 2022; Benamar et al., 2023; Khajmi et al., 2023).
The Marrakech-Safi region has a large number of radiology departments. These facilities are equipped to perform a range of imaging procedures and to provide essential medical imaging services to the local population; however, no dosimetric investigation has been carried out to analyze the X-ray doses administered in the region’s radiology departments.
This research was performed to evaluate the exposure parameters selected for radiographic examinations of adult patients and to estimate the entrance surface dose delivered to patients undergoing common diagnostic radiographic projections in the conventional radiology department of the Arrazi Hospital at the Med VI UHC in Marrakech, Morocco. Additionally, we aim to propose typical DRLs values for general radiography examinations. The outcomes of this study will contribute to the limited information currently available on radiation doses to adult patients from medical radiography in Morocco. The results will help clinicians understand the importance of using DRLs as a valuable tool for managing radiation doses in diagnostic radiology and will serve as a basis for further research.
2 Materials and methods
2.1 Patient exams and dosimetric calculations
This study was conducted prospectively. Picture Archiving and Communication Systems (PACS) were utilized to collect, store, and categorize data for each examination on a computer using a Microsoft Excel spreadsheet. The study included 1170 radiography exams of adult patients (over 18 yr of age), with radiographs sampled between March and July 2022. In this paper, we focused on patients with an average weight of 70 kg to evaluate the typical dose administered to an average patient. This audit of entrance surface dose estimation excluded patients who weighed less than 60 kg or more than 80 kg. Table 1 shows the number of conventional radiology examinations carried out and the exposure factors involved.
The conventional emergency radiology department at the ARH of Med VI UHC is equipped with a Philips digital tube diagnostic system, which has been in operation since 2016. It uses a flat sensor as an X-ray detector and regular maintenance is carried out to ensure optimal performance and the production of high-quality images, enabling accurate diagnosis and improved patient care. Dose assessment was performed on patients undergoing the eight most common diagnostic radiographs, which include twelve individual projections. These projections cover the following areas: cervical spine (AP/LAT), lumbar spine (AP/LAT), abdomen (AP), pelvis (AP), shoulder (AP), knee (AP/LAT), skull (AP/LAT) and chest (AP). Each radiograph was performed in the same radiology department.
Number of radiography projections, minimum, maximum, mean values of tube potential (kV), tube current (mAs), and exposure time (ms) of technical parameters for studied radiographic examinations.
2.2 Dose calculations
The dosimetry of the patients was carried out according to the projection using both the Dose Area Product (DAP) and the Entrance Surface Dose (ESD). The DAP is calculated by multiplying the radiation dose in air by the area of the X-ray field and is measured in mGy.cm2. This value is computed automatically for each exposure. DAP is used to assess the radiation doses administered to patients. These measurements are routinely displayed on the X-ray console for each examination. The following formula was used to estimate the ESD (Leclet, 2016):
IF is the irradiation field in cm2, and BSF is the backscattered factor. As per the study of Leclet in 2016 (Leclet, 2016), BSF is equivalent to 1.35 for voltages ranging from 60 to 80 kV and 1.5 for voltages over 80 kV.
2.3 Statistical assessment
The data was organized for analysis using Microsoft Excel 2019. Typical DRL values were computed as median distributions for each radiographic examination, in line with the International Commission on Radiological Protection Publication 135 (ICRP, 2017). Descriptive statistics, including the mean, median, 50th percentile, and 75th percentile values of the dosimetric variable of ESD, were utilized to evaluate the information. Additionally, the minimum, maximum, and average values of voltage (kV) and intensity (mAs) were calculated. We conducted a thorough analysis by comparing the TDRLs values with DRLs from significant studies carried out around the world: in France in 2013 (Roch et al., 2013), throughout the European Union in 2014 (EC, 2014), in the United Kingdom in 2016 (UK, 2016), in Nigeria in 2017 (Joseph et al., 2017), in Iran in 2020 (Hoseini et al., 2020), and in Ghana in 2023 (Gyan et al., 2023). This comprehensive comparison highlights the relevance of our findings within the context of international standards and practices.
3 Results and discussion
In this study, we examined all the radiographs performed in the radiology department of the Arrazi hospital over a five-month period during the year 2022, in order to determine the TDRL values, in line with the description of the different DRL categories in ICRP135 (ICRP, 2017).
The total number of adult patients included in this research is 1170. 62% (n = 756) were men, and 38% (n = 414) were women. Figure 1 shows that the most common radiographs are chest, knee and abdominal radiographs with a percentage of 30%, 19% and 10% respectively. Radiographs of the pelvis, lumbar spine, cervical spine and skull did not exceed 7%. For each of the eight radiographs, the average tube potential (kVp), tube current (mAs) and exposure time (ms) were obtained and are presented in Table 1. The minimum and maximum age criteria for all examinations were 19 and 84 yr, respectively. For the kV, the range is 44 kV to 125 kV; for the mAs, the range is 1 mA to 113 mAs; and for exposure time in milliseconds, the range is 1 ms to 208 ms. The large ranges of kV, mAs and ms were caused by the significant variations in patient size, weight, height and radiographic techniques used by radiology technicians. The documented technical radiographic parameters show that there are variations in technical factors when compared to the recommendations of the European Commission Quality Criteria (EC, 1996). Table 3 summarizes the calculated mean and the 50th and 75th percentiles of the entrance surface dose in mGy for each projection and examination considered.
For all examinations and projections, the estimated mean ESD ranged from a minimum of 0.24 mGy to a maximum of 4.59 mGy. Whereas the established typical DRL values for the entrance surface doses of all radiography projections were 1.52 mGy, 1.46 mGy, 3.34 mGy, 4.76 mGy, 1.56 mGy, 1.98 mGy, 1.25 mGy, 0.58 mGy, 0.58 mGy, 2.2 mGy, 2.1 mGy, and 0.22 mGy, for cervical spine AP, cervical spine LAT, lumbar spine AP, lumbar spine LAT, abdominal X-ray AP, pelvis X-ray AP, shoulder AP, knee AP, knee LAT, skull AP, skull LAT, and chest PA, respectively.
The typical DRL of ESD of 4.76 mGy for lumbar spine LAT radiography is higher than the other values. This is due to higher exposure parameters (i.e., kVp and mAs) than for the other examinations. The field size is another factor influencing the diagnostic reference level, which is larger for the abdomen than for the other radiographs. The chest X-ray AP projection had the lowest TDRL of ESD at 0.22 mGy, indicating lower exposure compared to the other radiographs.
In this study, the TDRL of the cervical spine AP and LAT (1.52 mGy/1.46 mGy), the knee AP and LAT (0.58 mGy/0.58 mGy), and the skull AP and LAT (2.2 mGy/2.1 mGy) are approximately identical; the discrepancy does not exceed 4%. This indicates that the radiology technicians at Arrazi hospital do not change the acquisition parameters between AP and LAT projections for these examinations. However, because the patient width is greater in the LAT position than in the AP position, the TDRL of 4.76 mGy of the LAT lumbar spine is 142% higher than in the AP lumbar spine of (3.34 mGy). In comparison of the median value of ESD for the abdominal X-ray (1.56 mGy) AP projection and the pelvic X-ray (1.98 mGy) AP projection, the TDRL value of the pelvic X-ray AP projection is 26% higher. For the shoulder X-ray AP projection, Table 2 shows that the TDRL (1.25 mGy) is 82% higher than that for the chest X-ray AP projection (0.22 mGy). The use of a high mAs (1–85 mAs) and kilovolt (50–77 kV) in this radiography could be behind the high dose delivered to the patients.
The high dose values observed in certain examinations in our survey may be due to inadequate training of imaging staff or to variations in technical parameters, clinical complexity of patients, and untimely quality control programs. The above finding is not unique to this study, this is confirmed by a study in Ghana (Ofori, 2013) and Nigeria (Joseph et al., 2017), but is common in other developing countries (Johnson et al., 2000; Wall et al., 2001; Kings et al., 2002).
The quantity of DRLs is contingent on numerous factors that influence patient exposure. The kVp has an effect on both the quantity and quality of the radiation beam, and for all radiography devices, the output increases with increasing kVp, resulting in a higher dose to the patients. The exposure is directly proportional to the mAs parameter, and the scattered radiation will increase with a larger field and impose more surface doses. The focal spot-to-surface distance (FSD) factor could also affect radiation exposure to patients. The operator’s selection of settings, as outlined above, is a pivotal factor in determining the absorbed dose. The expertise and dedication of the operator in utilizing appropriate settings can significantly influence the outcome. Reducing patient dose while maintaining image quality is achievable through routine staff training.
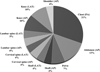 |
Fig. 1 Frequency distribution of radiographs studied. |
The calculated entrance surface dose (ESD) for all projections and examinations.
4 International comparison of DRLs
Table 3 shows the comparison of established typical diagnostic reference level values for radiographic examination with data from France in 2013 (Roch et al., 2013), the European Commission in 2014 (EC, 2014), the United Kingdom in 2016 (UK, 2016), Nigeria in 2017 (Joseph et al., 2017), Iran in 2020 (Hoseini et al., 2020), and Ghana in 2023 (Gyan et al., 2023).
The typical DRL value for the AP/LAT cervical spine of (1.52 mGy/1.46 mGy) was found to be higher than the values recorded in Nigeria of (0.62 mGy/0.79 mGy) and Ghana of (0.3 mGy/0.3 mGy) but lower than those of Iran of (1.6 mGy/1.7 mGy), France of (4 mGy/4 mGy), and EC of (4 mGy/7 mGy).
The median value of ESD for the AP/LAT lumbar spine of (3.34 mGy/4.76 mGy) in this analysis was lower than that seen in France of (10 mGy/25 mGy), in EC of (5 mGy/8 mGy), in the UK of (5.7 mGy/10 mGy), and in Iran of (5.3 mGy/11.8 mGy). However, it exceeds the registered DRL in Nigeria (1.22 mGy/1.59 mGy) and Ghana (1.6 mGy/3.1 mGy). This discrepancy can be attributed to the radiography techniques employed.
The established typical DRL values for abdominal and pelvic X-ray AP projection of 1.56 mGy–1.98 mGy were observed to be considerably lower than the values recorded values in France of 8 mGy–9 mGy, EC of 3 mGy–4 mGy, UK of 4 mGy–4 mGy, and Iran of 4.3 mGy–3.2 mGy, but higher when compared to Nigeria of 1.01 mGy–0.82 mGy and Ghana of 1.3 mGy–0.92 mGy. This could generally be linked to the technology used.
The typical value of the entrance surface dose presented here for the shoulder AP projection of 1.25 mGy is well above the statistics of other studies. This demonstrates that higher exposure parameters are used for this radiography because of the greater thickness in this part of the body. The TDRL value of this work based on ESD for knee AP projection is 0.58 mGy. This is higher than the DRL values for the EC (0.4 mGy), the UK (0.3 mGy), and Nigeria (0.5 mGy). Whereas, expect DRL in the UK during 2016 for knee LAT projection; the median value of ESD is lower. Regarding skull AP/LAT, the DRL values of 2.2 mGy/2.1 mGy were higher than those published in the other countries, with the exception of France’s 2013 estimate of 3 mGy/5 mGy and Iran’s 2022 value of 2.2 mGy/2.4 mGy. For chest X-ray PA projection, the TDRL in this study was found to be 0.22 mGy higher than that seen in the UK (0.15 mGy) but less than those registered in France (0.3 mGy), EC (0.3 mGy), Nigeria (0.59 mGy), Iran (1.4 mGy), and Ghana (0.3 mGy).
Table 3 shows that there are differences between our study’s TDRLs and those of official organizations (EC, 2014) and the other reporting nations. The variations in dosage between the research centers are consistent with the results of Shrimpton et al. (1986), who revealed that disparities between the centers might reach up to 10 to 40 in the UK and 8 to 20 in Norway. The radiography technology system may be responsible for these variances. Different DRLs in such an inter-survey comparison will result from a range of causes, including statistical variances, measuring techniques, clinical approaches, and equipment. For example, the French (Roch et al., 2013) and UK (UK, 2016) surveys during 2013 and 2016 selected patient dosage data from a large number of institutions of different sizes. Besides, a very large number of hospital radiological examination doses were also reviewed. In Nigeria (Joseph et al., 2017), the study was conducted in two university teaching hospitals, and 750 patients were assessed. While all 1170 radiographs in our investigation were conducted in a single digital radiography room with one X-ray machine.
Comparison of the TDRL result of each examination with the relevant ESD (mGy) literature.
5 Conclusion
This project developed typical DRLs values in terms of ESD for eight radiographic examinations at the Mohammed VI University Hospital Centre at the Arrazi Hospital in Marrakech, Morocco. An evaluation of local practices, taking into account operational procedures or equipment performance. The findings demonstrated that, with the exception of the TDRLs of the shoulder, knee, and skull radiographs, which were greater than those published elsewhere, most of the DRLs were lower than the suggested international DRLs.
In order to minimize the risk of stochastic effects associated with radiography, the X-ray department of the Arrazi Hospital requires a process of homogenization of radiation exposure to patients undergoing radiographic examinations, regular quality control of equipment, and a dose optimization strategy.
To establish a baseline, the information collected in this study can be compared to future dose assessments. Authorities at the national and professional levels might also find this dose survey helpful to develop the national DRLs for conventional radiography in Morocco.
Acknowledgments
The authors would like to express their gratitude to everyone who provided assistance throughout this study, particularly the radiography center for their cordial collaboration.
Funding
The study’s authors did not receive any funding for it.
Conflicts of interest
There is no conflict of interest for this paper.
Data availability statement
The entire study results are available from H. KHAJMI, the corresponding author.
Author contribution statement
Each author contributed to the study’s design and implementation, analysis of the results, and writing of the report.
Ethics approval
Ethical approval was not required.
Informed consent
This study did not require informed consent.
References
- Alrehily F. 2022. Diagnostic reference levels of radiographic and ct examinations in Saudi Arabia: A systematic review. Radiat Prot Dosim 198 (19): 1451–1461. https://doi.org/10.1093/rpd/ncac183. [Google Scholar]
- Benamar M, et al. 2023. Patient dose assessment in computed tomography in a Moroccan imaging department. Radioprotection 58 (1): 49–53. https://doi.org/10.1051/radiopro/2022039. [CrossRef] [EDP Sciences] [Google Scholar]
- Benmessaoud M, et al. 2021. Derivation of local diagnostic reference levels for common adult computed tomography examinations in Moroccan hospital. Radiat Prot Dosim 194 (4): 208–213. https://doi.org/10.1093/rpd/ncab095. [Google Scholar]
- Ciraj O, et al. 2005. A survey of patient doses from conventional diagnostic radiology examinations: first results from Serbia and Montenegro. Phys Med 21 (4): 159–163. [Google Scholar]
- EC European Commission. 2014. Radiation Protection No. 180. https://ec.europa.eu/energy/sites/ener/files/documents/RP180%20part2.pdf. [Google Scholar]
- EUR96 European Guidelines on Quality Criteria for Diagnostic Radiographic Images, European Commission, EUR 16260 EN, June 1996. [Google Scholar]
- El Mansouri M, et al. 2022. Establishing local diagnostic reference levels for adult computed tomography in Morocco. Radioprotection 57 (1): 61–66. https://doi.org/10.1051/radiopro/2021035. [CrossRef] [EDP Sciences] [Google Scholar]
- European Commission. 1999. Radiation protection report 109. Guidance on diagnostic reference levels (DRLs) for medical exposures. European Commission, UK. [Google Scholar]
- European Commission (EC): Diagnostic Reference Levels in Thirty-six European Countries Part 2/2. Radiation protection No.180. Luxembourg: Publications Office of the European Union, 2014. [Google Scholar]
- France IRSN PRP-HOM. 2020. Analyse des données relatives à la mise à jour des niveaux de référence diagnostiques en radiologie et en médecine nucléaire. Bilan 2016–2018. Rapport parut en 2020. [Google Scholar]
- Gyan E, et al. 2023. Proposed institutional diagnostic reference levels in computed and direct digital radiography examinations in two teaching hospitals. J Radiat Prot Res. https://doi.org/10.14407/jrpr.2021.00367. [Google Scholar]
- Hart D, et al. 2009. National reference doses for common radiographic, fluoroscopic and dental X-ray examinations in the UK. NRPB-R200. Br J Radiol 82 (973): 1–12. https://doi.org/10.1259/bjr/12568539. [Google Scholar]
- Hart D, et al. 2012. Doses to patients from radiographic and fluoroscopic X-ray imaging procedures in the UK − 2010 review. HPA-CRCE-034. [Google Scholar]
- Hoseini Motlagh Z, et al. 2020. Determination of diagnostic reference level in routine examinations of digital radiography in Mazandaran province. Radiat Prot Dosim 190 (1): 31–37. https://doi.org/10.1093/rpd/ncaa074. [Google Scholar]
- ICRP. 1996. Publication 73, annals of the ICRP 26, recommendations of the international commission on radiological protection. Oxford: Pergamon Press. [Google Scholar]
- International Commission on Radiological Protection (ICRP). 2017. Diagnostic reference levels in medical imaging. ICRP Publication 135. Ann. ICRP 46 (1): 1–144. [Google Scholar]
- International Atomic Energy Agency. Dosimetry in diagnostic cradiology: an international code of practice. Technical Reports Series No. 457 (Vienna: IAEA) (2007). [Google Scholar]
- Johnson, et al. 2000. Reference dose levels is for patients undergoing common diagnostic X-rays examination in Irish Hospitals. British J Radiol 73: 396–402. https://doi.org/10.1259/bjr.73.868. 10844865. [Google Scholar]
- Joseph DZ et al., 2017. Establishment of Local Diagnostic Reference Levels (DRLs) for Radiography Examinations in North Eastern Nigeria. Sci World J 12 (4). [Google Scholar]
- Khajmi H, et al. 2023. Evaluation of X-ray doses in pediatrics multislice computed tomography. Radioprotection. https://doi.org/10.1051/radiopro/2023029. [Google Scholar]
- King S, et al. 2002. Optimizing medical radiation exposures for uroradiological procedures, with special emphasis on paediatric imaging. BJU Int 89 (6). https://doi.10.1046/j.1464-410X.2002.02660.x. [Google Scholar]
- Leclet H. 2016. La métrologie des niveaux de dose dans les pratiques radiodiagnostiques. http://www.bivi.metrologie.afnor.org [Google Scholar]
- MedizinischeStrahlenschutzverordnung, Verordnung der Bundesministerinfür Gesundheit und Frauen überMaßnahmenzum Schutz von PersonenvorSchädendurchAnwendungionisierenderStrahlungimBereich der Medizin, BGBl. II Nr. 197/2010, (2010). Germany. [Google Scholar]
- Metaxas VI, et al. 2019. Patient doses in common diagnostic X-ray examinations. Radiat Prot Dosim 184 (1): 12–27. https://doi.org/10.1093/rpd/ncy169. [Google Scholar]
- Mohsenzadeh B, et al. 2020. Assessment of patient dose in routine digital radiography in Iran. Int J Radiat Res 18 (3): 449–460. https://doi.org/10.18869/acadpub.ijrr.18.3.449. [Google Scholar]
- Ofori EK. 2013. Radiology & imaging. Radiology 2013. https://doi.org/10.4172/2167-7964.S1.002. [Google Scholar]
- Roch P, et al. 2013. French diagnostic reference levels in diagnostic radiology, computed tomography and nuclear medicine: 2004-2008 review. Radiat Prot Dosimetry 154: 52–75. https://doi.org/10.1093/rpd/ncs152. [CrossRef] [PubMed] [Google Scholar]
- Shrimpton PC, et al. 1986. National survey of doses to patients undergoing a selection of routine X-ray examination in english hospitals. NRBP- R 200: Chilton, UK. [Google Scholar]
- Talbi M, et al. 2022. Local Diagnostic Reference Levels (LDRLs) for routine X-ray examinations in Morocco. Radioprotection 57 (2): 149–155. https://doi.org/10.1051/radiopro/2022008. [CrossRef] [EDP Sciences] [Google Scholar]
- UK. 2016. https://www.gov.uk/government/publications/diagnostic-radiology-national-diagnostic-reference-levels-ndrls/ndrl. Accessed 2-9-2024. [Google Scholar]
- United Nations Scientific Committee on the Effects of Atomic Radiation. Sources and effects of ionizing radiation: report to the General Assembly, annex D, medical radiation exposures. New York, NY: United Nations, 2000. [Google Scholar]
- Wall BF. 2001. Diagnostic reference levels −the way forward. British J Radiol 74 (885): 785–788. https://doi.org/10.1259/bjr.74.885.740785. [Google Scholar]
- Ziliukas JL, et al. 2010. Management of patient doses and diagnostic reference levels in X-ray radiography in Lithuania. Radiat Prot Dosim 139 (1-3): 313–316. https://doi.org/10.1093/rpd/ncq102. [Google Scholar]
Cite this article as: Khajmi H, Tounsi A, Oufni L. 2026. Estimation of entrance surface dose for radiography examinations in Arrazi Hospital from Mohammed VI University Hospital Center of Marrakech (Morocco). Radioprotection 61(2): 126–131. https://doi.org/10.1051/radiopro/2025028
All Tables
Number of radiography projections, minimum, maximum, mean values of tube potential (kV), tube current (mAs), and exposure time (ms) of technical parameters for studied radiographic examinations.
Comparison of the TDRL result of each examination with the relevant ESD (mGy) literature.
All Figures
|
Fig. 1 Frequency distribution of radiographs studied. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.