")
")
| Issue |
Radioprotection
Volume 53, Number 4, October-December 2018
|
|
|---|---|---|
| Page(s) | 279 - 286 | |
| DOI | https://doi.org/10.1051/radiopro/2018033 | |
| Published online | 10 décembre 2018 | |
Article
Radiation exposure of very-low-birth-weight infants in neonatal intensive care units in Korea
1
Department of Pediatrics, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine,
170 Jomaru-ro,
Bucheon
14584, Republic of Korea
2
Departments of Radiology, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine,
170 Jomaru-ro,
Bucheon
14584, Republic of Korea
* Corresponding author: Cette adresse e-mail est protégée contre les robots spammeurs. Vous devez activer le JavaScript pour la visualiser.
Received:
26
April
2018
Accepted:
14
September
2018
Abstract
To our knowledge, no study has reported the radiation doses of neonates admitted to neonatal intensive care units (NICUs) in Korea. Therefore, we evaluated the radiation frequency and dose of radiation performed in NICUs using mobile X-ray machines. We retrospectively analyzed the number of radiographs and doses among 290 very low-birth-weight infants (VLBWIs) admitted at our hospital between 2011 and 2016. We compared X-ray frequencies and radiation doses according to clinical characteristics and morbidities. The entrance surface doses (ESDs) were calculated using the non-dosimeter dosimetry formula. The median number of radiographs per infant was 26, and about 25% neonates had over 50 radiographs. The number of radiographs taken was higher for infants with low-birth-weight (LBW), respiratory distress syndrome, bronchopulmonary dysplasia, and longer central venous catheterization duration (p < 0.001 for all). The cumulative ESD was 0.18 to 9.89 mGy, and the ESD per radiograph was 0.049 to 0.069 mGy. The LBW and the more severe the neonates’ condition, the greater was the radiation exposure. It is difficult to reduce the number of radiographic examinations, but the quality of examinations must be improved without compromising patient care. Additional studies are needed to minimize the cumulative exposure dose and achieve optimal image quality.
Key words: neonatal intensive care units / radiation dose / low-birth-weight infant
© EDP Sciences 2018
1 Introduction
Owing to advances in neonatal intensive care, including radiologic examination, it has become possible to diagnose, assess, and even treat various diseases earlier than before. Thus, more preterm babies with low gestational age and low-birth-weight (LBW) have survived (Chang, 2016). According to data from the Statistics Korea (2016), 21 355 LBW infants (birth weight < 2.5 kg) were born in 1996, accounting for 3.08% of total births, and this value increased to 5.8% in 2016. Meanwhile, only 1205 very LBW infants (VLBWIs, birth weight < 1.5 kg) were born in 1996, and this number increased by about 1700 to reach 2883 in 2016 (Statistics Korea, 2016). The proportion of VLBW births has increased from 0.17% to 0.68% in 20 years (Statistics Korea, 2016).
The major risk of concern for an irradiated neonate is childhood cancer. Preterm neonates are more affected by radiation than older children and adults (Datz et al., 2008) because they have a longer remaining life expectancy and are more inherently radiosensitive than others. Additionally, preterm infants are more vulnerable to immediate and long-term morbidities and mortality than term neonates, so they need to undergo radiography multiple times (Donadieu et al., 2006; Manuck et al., 2016). For example, infants with complications such as bronchopulmonary dysplasia (BPD) may require additional examinations after discharge. Another reason is that because of their small size, preterm infants receive more radiation exposure than needed. The small size of premature infants places all their organs within the range of radiation, resulting in a higher effective dose than in children and adults. Although X-ray has become indispensable in neonatal intensive care unit (NICU) for diagnosis, treatment, and status monitoring, the X-ray has been often overused because of their ease of use and usefulness. Thus, the amount of radiation infants receive and the effect of diagnostic radiation must be carefully considered. The number of X-ray examinations performed on preterm neonates has been described in several studies (Ono et al., 2000, 2003; Datz et al., 2004; Donadieu et al., 2006; Bader et al., 2007; Puch-Kapst et al., 2009; Yu, 2010). Donadieu et al. (2006) reviewed all preterm infants (gestational age < 34 weeks) in a NICU and found that the cumulative doses received were within the range of environmental ionizing radiation received over a similar period (United Nations Scientific Committee on the Effects of Atomic Radiation, 2000). Ono et al. (2000) found that LBW infants needed a longer duration of hospitalization and more radiological examinations than those with normal birth weight.
To the best of our knowledge, no study has reported the radiation doses received by neonates admitted to NICUs in Korea. In the present study, we assessed the number of X-ray examinations performed on preterm infants and the resulting patient radiation exposure as functions of patient weight and patient morbidity. These indicators can help neonatal facilities to optimize their practice for patient radioprotection.
2 Material and methods
2.1 Patients and methods
This study was approved by the Institutional Review Board of the Soonchunhyang University Bucheon Hospital May 29, 2017 and conducted according to the guidelines of the Declaration of Helsinki.
We retrospectively reviewed the medical records of 290 VLBWIs (< 1500 g) admitted to the NICU of the Soonchunhyang University Bucheon Hospital between January 1st, 2011, and December 31st, 2016. This NICU is a level III NICU and cares for about 400 neonates annually. The total number of beds in the NICU was 17 in 2011, and it was expanded to 27 beds in 2015 thanks to government funding. Infants who were transferred to another hospital (n = 23), died during hospitalization (n = 35), and were admitted for more than 1 year (n = 1) were excluded. A flowchart illustrating the course of the study is presented in Figure 1. One patient who was excluded from the study was born at 27 weeks of gestational age with a birth weight of 810 g and had multiple complications including hydrocephalus and short bowel syndrome. He was admitted for 395 days and underwent surgery for hydrocephalus and necrotizing enterocolitis (NEC). He underwent several radiological procedures, including two small bowel series, four brain computed tomography (CT) scans, and 286 plain radiographs.
Patients were classified by birth weight into four groups: ≤ 750 g, 751 to ≤ 1000 g, 1001 to ≤ 1250 g, and 1251 to ≤ 1500 g to compare the radiation exposure among these groups. To evaluate gonad exposure, we analyzed the frequency of gonad exposure on X-ray images.
We evaluated the following clinical characteristics: gestational age, birth weight, mode of delivery, gender, duration of hospitalization, Apgar score at 1 and 5 minutes, oxygen supply method, central line insertion duration, and total parenteral nutrition duration. The neonatal morbidities reviewed were respiratory distress syndrome (RDS), patent ductus arteriosus (PDA), BPD, early-onset sepsis (EONS), late-onset sepsis (LONS), NEC (stage ≥ 2), intraventricular hemorrhage (IVH) (grade ≥ 1), retinopathy of prematurity (ROP) (stage ≥ 1), pneumothorax, and periventricular leukomalacia (PVL).
RDS was defined by the presence of characteristic radiographic findings and oxygen requirement without any evidence of another cause of respiratory distress. BPD was defined as the need for supplemental oxygen at 36 weeks of postmenstrual age (Jobe and Bancalari, 2001). EONS was defined as sepsis in the first 3 days of life, while LONS was defined as sepsis occurring after 72 hours in NICU infants and after 7 days of life in term infants (Hornik et al., 2012).
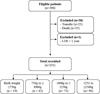 |
Fig. 1 Study flow. LOS: length of stay. |
2.2 Imaging technique
Most of the patients were laid in the incubator of the NICU and the image detector was placed directly under the patients when they got X-ray examinations. In the case of the incubator with a system drawer, this system drawer was used for scanning. All radiographic images were recorded using the mobile X-ray machine (MUX-100H; Shimadzu, Tokyo, Japan) in the NICU. It used a phosphor X-ray converter and the type of detector is image plate. The X-ray unit consists of an inverter type generator with 2.5 mm aluminum filtration (1.5 mm of aluminum in the tube and 1.0 mm in the collimator). According to patients birth weight, we used following parameters when they got X-ray examinations (Tab. 1), and in some X-rays, tube voltage and tube current were selected specifically for neonates by the radiographer’s decision, considering their weight and body sizes. In the NICU, the range of applied tube potential values was 50 to 65 kVp, and that of tube current time product values was 0.8 to 1.8 mAs. Fields size was variable and adjusted according to patient size. If we take chest AP radiography, field size is about 6 × 6 inches and IP plate size was 10 × 12 inches. All the film-to-skin distances (FSD) were set between 80 and 100 cm.
We used a 1-mm lead sheet covered with polyvinyl chloride over the gonads to reduce gonad exposure. According to the policy of our hospital, the gonad protector should be applied in all abdomen and pelvic examinations at the NICU, for all male and female infants. While taking X-ray for evaluation of the bowel gas pattern, the gonad shield was not used.
We opened all the X-ray files directly, visually confirming the gonad exposure of each infant. For male patients, the placement of the protector was considered appropriate if the shield fully covered the testes. For female patients, the placement was considered appropriate when the shield covered the pelvic basin from the symphysis pubis to the sacrum without covering the bony landmarks (Lee et al., 2017).
Details of the parameters used for each patient weight group.
2.3 Estimation of the patient radiation exposure
Entrance surface dose (ESD) has been widely used as an indicator to monitor radiation exposure because it is easy to measure (Smans, 2009; Vachharajani et al., 2013). Direct measurement of ESD using thermoluminescent dosimeters and dose-area product (DAP) meters is the most accurate method to measure exposure dose. However, radiation dose is not routinely measured in premature babies, and only few facilities are equipped with DAP meters. Therefore, mathematical equations have been suggested by several studies to calculate the radiation dose from radiographic examinations, and some reports have shown that the calculated value corresponds to direct measurement value in radiographic examinations (Ishiguchi et al., 2000; Kim et al., 2005). Since we use a mobile X-ray machine that cannot measure DAP, we calculated the ESD using the non-dosimeter dosimetry method developed by Mori (Ibaragi Radiological Technologists Association et al., 1996) and compared our findings with those of other studies and reference values (Sutton et al., 1998; Ono et al., 2003; Donadieu et al., 2006; Bader et al., 2007; Baert et al., 2008; Puch-Kapst et al., 2009). The non-dosimeter dosimetry-M equation calculates the ESD according to the rectification method of the photographic equipment. The ESD through a three-phase full-wave rectification is calculated as follows (Ibaragi Radiological Technologists Association et al., 1996; Sung et al., 2016):

ESD: entrance surface dose (mGy)
kV(f): tube potential correction factor
f: total filtration correction factor
mAs: tube current-time product
FSD: film-to-skin distance (m)
0.88 × 10−2: absorbed dose conversion factor.
We calculated the ESD by substituting all the parameters directly into the equation. According to the literature, in the case of single-phase full-wave rectifier circuit X-ray generator and inverter-type X-ray generator, the ESD is multiplied by 0.55 and 0.95, respectively (Sung et al., 2016). Because the X-ray used in our hospital is from an inverter type X-ray generator, the ESD calculated by the above equation was multiplied by 0.95. We reviewed all radiographic X-rays (abdomen, chest, and skeletal plain films; contrast-enhanced films of the gastrointestinal system) and recorded the number of mobile X-ray films and exposure parameters [kV(f), mAs, and FSD] performed during hospital stay. All data were double checked, and no data were missed.
2.4 Statistical analysis
Data were expressed as median (interquartile range) for quantitative variables and n (%) for qualitative variables. Group comparisons were conducted using the Jonckheere-Terpstra test for quantitative variables and Mantel-Haenszel’s linear-by-linear trend test or Chi2 test for qualitative variables. We used uni- and multivariate logistic regression to examine potential risk factors for high ESD. Significant variables with p < 0.05 in the univariate analysis were selected for the multivariate regression analysis, which was performed using the stepwise backward method (likelihood ratio). The variables that continued to have p-values ≤ 0.05 after adjustments were retained in the multivariate regression model. A level of p < 0.05 was considered significant. All statistical analyses were performed using R (version 3.3.2; The R Foundation for Statistical Computing, Vienna, Austria).
3 Results
The clinical characteristics of the patients are presented in Table 2. Since the number of radiographs was markedly skewed to the right (Fig. 2), we used the median value when summarizing the number of radiographs for each group. Of the 231 infants included (range of birth weight: 470–149 g), the median gestational age and birth weight were 29.1 weeks and 1200 g, respectively. The number of boys was 114 (49.4%), and no significant differences were found in sex among groups. The infants were diagnosed with RDS, PDA, BPD, EONS, LONS, NEC, IVH, ROP, pneumothorax, and PVL, all of which are largely associated with prematurity. RDS was diagnosed in 75.3% of the patients and BPD, in 40.7%. As the birth weight of the infants increased, the rate of morbidities, except EONS, pneumothorax, and PVL, decreased.
The total number of X-ray examinations was the highest for infants with birth weight ≤ 750 g, at 77, followed by the group with birth weight 751 to ≤ 1000g (n = 50), 1001 to ≤ 1250 g (n = 28), and 1251 to ≤ 1500 g (n = 17.5) (p < 0.001 for trend). The most common X-ray examination was for the chest, including abdominal X-ray examinations (babygram). During the study period, 95.2% of premature infants weighing less than 1500 g were X-rayed under the setting conditions at 55 kVp and 1.6 mAs, except for 495 X-rays with precisely specified setting values. The cumulative estimated ESD varied between 0.18 and 9.89 mGy, and the ESD per radiograph ranged from 0.049 to 0.069 mGy. The calculated median cumulative ESD of preterm infants born at ≤ 750 g was 4.83 mGy, while that of preterm infants born at 1251 to ≤ 1500 g was 1.10 mGy (Fig. 3), and this difference was statistically significant (p < 0.001 for trend). Furthermore, the extent of gonad exposure differed significantly among the groups. The lower the birth weight, the significantly higher the gonad exposure rate (p < 0.001); the female infants tended to have a higher gonad exposure rate than the male infants (Tab. 3).
Linear regression analysis was conducted to identify the factors affecting total ESD (Tab. 4). According to the univariate regression analysis, all morbidities except for gender, EONS, and PVL differed significantly among the groups. After final selection, the birth weight, RDS, BPD, and duration of ventilation remained risk factors for high radiation exposure. The total ESD was −0.5 mGy [95% confidence interval (CI), −0.88 to −0.11] lower in neonates born at > 1250 g than those born at ≤ 750 g, and it was 0.44 mGy (95% CI, 0.24 to 0.65) higher in neonates with RDS than those without RDS. As the severity of BPD increased, the ESD increased (p < 0.001). The duration of ventilation was also significantly correlated with the total ESD (p < 0.001). As shown in Figure 3, the lower the birth weight, the higher was the calculated ESD (p < 0.001).
Baseline characteristics of patients grouped by birth weight (≤ 750 g, 751 to ≤ 1000 g, 1001 to ≤ 1250 g, 1251 to ≤ 1500 g).
 |
Fig. 2 Distributions of radiographs in each birth weight group. |
 |
Fig. 3 Entrance skin dose for each birth weight groups. |
Radiation-related characteristics according to birth weight.
Linear regression analysis for cumulative entrance skin dose in neonates.
4 Discussion
Medical advances were achieved owing to the accessibility to X-ray examinations and more preterm neonates can survive than before. Although benefit from radiologic procedures will outweigh the risk of the exam, it is necessary to know the present state of radiologic procedures and propose dose optimization strategy.
Generally, the tube voltage (41–62 kVp) and current time product (0.5–4 mAs) used vary widely across centers (Bahreyni Toosi and Malekzadeh, 2010). The analysis of radiographic parameters in the present study showed that in most cases, the X-ray tube voltage (kV) used for plain radiographs was lower than that suggested by the Commission of the European Communities, at between 60 and 65 kVp (European Commission, 1996). Additionally, we took an X-ray at a distance of 80 to 100 cm, which is consistent with the 80 to 100 cm recommended for newborn radiography by the European Guidelines (European Commission, 1996). The median ESD value (0.06 mGy) was higher than those proposed by the National Radiological Protection Board (50 µGy) (Hart et al., 2000) for neonatal chest X-ray examination, but lower than those proposed by the guidelines of the European Commission (80 µGy, European Commission, 1996). Our findings showed that the median ESD values or the number of X-ray procedures performed for each neonate were higher than those reported previously (Sutton et al., 1998; Ono et al., 2003; Donadieu et al., 2006; Bader et al., 2007; Baert et al., 2008; Puch-Kapst et al., 2009). Although low voltage–high tube current time product combination shows good image quality, it could lead to high ESD (Frayre et al., 2012; Porto et al., 2014). Therefore, the use of low tube voltage techniques and lack of specialized neonatal radiologic technicians may explain the higher ESD in our study.
Early in the present study, we had not considered the effects of radiation when X-rays were applied. Because the babygram was more useful in identifying the overall status of neonates, rather than chest X-rays or abdomen X-rays alone, the babygram was commonly applied in practice, rather than focusing on areas that pediatricians were interested in. Soboleski et al. (2006) reported that 43% of chest radiographs for pediatric patients and neonates showed non-thoracic structures, and Datz et al. (2008) concluded that 50% of the effective radiation dose results from unintentional exposure and can be reduced by suitable examinations. We have to carefully consider the selection of the area covered by radiographic examination and use proper collimation in order to reduce radiation exposure to non-relevant organs.
It is well-known that the hematopoietic system and gonads are radiosensitive, while the central nervous system and liver are relatively radioresistant (Yu, 2010). To protect the gonads during radiologic examination in neonates, application of a gonad shield has been widely accepted since the mid-1950s (Fawcett and Barter, 2009). Several studies have examined the application of a gonad shield (Bader et al., 2007). Fawcett and Barter (2009) reported that the protector was accurately placed in only 26% of cases, and the proportion of correctly placed shields was lower in girls than in boys, which is consistent with our findings. Because of their anatomical location, the ovaries are not fully covered, and sometimes gonad shields obscure the region of interest, causing repeated tests. The reasons why the neonates at our hospital experienced more gonad exposure were the lack of awareness about the effect of radiation on the gonads, the fact that neonates move rapidly, and technicians forgetting to shield the gonads during radiography. One study showed that the dose received by the gonads can be reduced by 30 to 40% if the shield containing lead equivalent material is correctly placed (McCarty et al., 2001). In other words, the “as low as reasonably achievable” principle should be kept in mind, and new landmarks need to be identified to ensure that essential diagnostic information is obtained while the gonads are accurately protected.
In the future, various efforts are required to reduce the radiation exposure to neonates in the NICU. First, from the clinician’s viewpoint, after determining the disease or morbidity that affects the number of X-ray examinations, clinicians should make efforts to reduce the radiologic intervention to the minimum influence level on the state of patients by lowering the TPN duration and ventilation duration, as well as the number of C-line insertions. Moreover, careful physical examination is required to justify the necessity of X-ray examination. The possibility of other radiation-free modalities should also be considered to help reduce the radiation dose. For instance, ultrasonography can be used to ensure the proper positioning of a central line tip instead of X-ray examination (Scott et al., 2014), or magnetic resonance imaging can be used instead of CT. Portable ultrasonography has been available in the NICU of our hospital since 2016 to determine the abdomen status whenever necessary, thus reducing the frequency of abdomen X-ray as well as the gonad exposure. Next, the radiologic technicians shall use appropriate parameters according to the patient’s weight and size, and appropriately use the gonad protector depending on the situations. Finally, on the system level, by training NICU-specialized radiographers regarding equipment quality control, image management, patient dose management, and radiation hazards, the homogeneity of practice among radiographers must be implemented. Gupta et al. (2015) conducted a study to improve the quality of radiographs by developing and implementing an educational tool that provides regular constructive feedback and is controlled by the clinical staff at the bedside. After intervention, significant improvements were obtained in image quality, such as optimal positioning and absence of artifacts.
Currently, NICU-dedicated DR equipment [Samsung Electronics, GM85, South Korea (manufactured in July 2017)] has been used in the hospital since June 19, 2017 to facilitate accurate ESD measurement. Therefore, more in-depth research can be performed henceforth.
Our study has several limitations. First, it is a single-institution study, and our findings may not be generalizable to other hospitals or the nation. Second, the calculated ESD was probably underestimated because we excluded patients who were transferred to other hospitals. These subjects may have undergone more radiographic examinations for complex problems. Next, we did not include radiation exposure from CT, esophagography, or other such procedures. The radiation doses and effects from these procedures are considerably higher than those from plain radiography (Fletcher et al., 1986; Donadieu et al., 2006), so this must be factored in when estimating long-term effects.
To our knowledge, this is the first study conducted to determine the radiation doses received by neonates in Korea whose birth weight is < 1500 g and ascertain the frequency and cumulative radiation dose of the procedures. These efforts should not be limited to VLBWI, and we should attempt to reduce the degree of radiation exposure in infants, older children, and adults. There is a continuous need to evaluate radiation exposure, our findings should be compared with those from other NICUs in Korea; furthermore, data gathering and long-term follow-up are required in order to understand the effect of radiation exposure from diagnostic procedures (Hall et al., 2004).
Acknowledgements
This study was made possible by support from neonatologists, the radiologists, and radiology technicians. The authors wish to thank them for their assistance and support. And this study was supported by the Soonchunhyang University Research Fund
References
- Bader D, Datz H, Bartal G, Juster AA, Marks K, Smolkin T, Zangen S, Kugelman A, Hoffmann C, Shani G, Ben-Shlomo A, Margaliot M, Sadetzki S. 2007. Unintentional exposure of neonates to conventional radiography in the Neonatal Intensive Care Units. J. Perinatol. 27(9): 579–585. [CrossRef] [PubMed] [Google Scholar]
- Baert AL, Knauth M, Sartor K. 2008. Radiological imaging of the neonatal chest. 2nd Ed. New York, Berlin, Heidelberg: Springer. [Google Scholar]
- Bahreyni Toossi MT, Malekzadeh M. 2010. Diagnostic reference levels in neonatal units. In: International symposium on standards, applications and quality assurance in medical radiation dosimetry (IDOS), Nov 9–12, AU (M.T. Bahreyni Toossi, M. Malekzadeh, Eds.) pp. 175–176. Vienna: International Atomic Energy Agency. [Google Scholar]
- Chang YS. 2016. Past, present, and future of neonatology in Korea. J. Korean Med. Assoc. 59(7): 487–489. [CrossRef] [Google Scholar]
- Datz H, Margaliot M, Ben-Shlemo A, Shani G, Bader D, Sadetzki S, Uster A, Marks K, Solomkin T, Zangen D. 2004. Neonates are over exposed to X-ray radiation during their stay in NICUs. In: Conference of the Nuclear Societies in Israel, Feb 17–18, 2004 (H. Datz, M. Margaliot, A. Ben-Shlemo, G. Shani, D. Bader, S. Sadetzki, A. Uster, K. Marks, T. Solomkin, D. Zangen, Eds.), p. 247. Tel Aviv, IL: The nuclear societies in Israel. [Google Scholar]
- Datz H, Ben-Shlomo A, Bader D, Sadetzki S, Juster-Reicher A, Marks K, Smolkin T, Zangen S, Margaliot M. 2008. The additional dose to radiosensitive organs caused by using under-collimated X-ray beams in neonatal intensive care radiography. Radiat. Prot. Dosim. 130(4): 518–524. [CrossRef] [Google Scholar]
- Donadieu J, Zeghnoun A, Roudier C, Maccia C, Pirard P, André C, Adamsbaum C, Kalifa G, Legmann P, Jarreau PH. 2006. Cumulative effective doses delivered by radiographs to preterm infants in a neonatal intensive care unit. Pediatrics 117(3): 882–888. [CrossRef] [PubMed] [Google Scholar]
- European Commission. 1996. European guidelines on quality criteria for diagnostic radiographic images in paediatrics. Luxembourg, LU: Office for official publications of the European Communities. [Google Scholar]
- Fawcett SL, Barter SJ. 2009. The use of gonad shielding in paediatric hip and pelvis radiographs. Br. J. Radiol. 82(977): 363–370. [CrossRef] [PubMed] [Google Scholar]
- Fletcher EW, Baum JD, Draper G. 1986. The risk of diagnostic radiation of the newborn. Br. J. Radiol. 59(698): 165–170. [CrossRef] [PubMed] [Google Scholar]
- Frayre AS, Torres P, Gaona E, Rivera T, Franco J, Molina N. 2012. Radiation dose reduction in a neonatal intensive care unit in computed radiography. Appl. Radiat. Isot. 71(Suppl.): 57–60. [Google Scholar]
- Gupta AO, Rorke J, Abubakar K. 2015. Improving the quality of radiographs in neonatal intensive care unit utilizing educational interventions. Am. J. Perinatol. 32(10): 980–986. [CrossRef] [PubMed] [Google Scholar]
- Hall P, Adami HO, Trichopoulos D, Pedersen NL, Lagiou P, Ekbom A, Ingvar M, Lundell M, Granath F. 2004. Effect of low doses of ionising radiation in infancy on cognitive function in adulthood: Swedish population based cohort study. BMJ 328(7430): 19. [Google Scholar]
- Hart D, Wall B, Shrimpton P. 2000. Reference doses and patient size in paediatric radiology. Didcot, UK: National Radiological Protection Board. [Google Scholar]
- Hornik CP, Fort P, Clark RH, Watt K, Benjamin DK, Jr, Smith PB, Manzoni P, Jacqz-Aigrain E, Kaguelidou F, Cohen-Wolkowiez M. 2012. Early and late onset sepsis in very-low-birth-weight infants from a large group of neonatal intensive care units. Early Hum. Dev. 88(Suppl. 2): S69–S74. [CrossRef] [PubMed] [Google Scholar]
- Ibaragi Radiological Technologists Association, Japanese Society of Radiological Technology, Ibaragi Branch, Radiation Exposure Reduction Committee. 1996. Simple conversion equation of entrance dose on patient skin surface in X-ray diagnosis area: NDD method. Mito, JP: Japan Society of Radiological Technology, Ibaraki Branch. [Google Scholar]
- Ishiguchi T, Iwanami S, Kawatsu S, Ishigaki T, Koga S. 2000. Radiation exposure by routine radiographic examinations: multicenter study in Japan with thermoluminescence dosimetry and estimation from the radiographic data. In: International Congress of the International Radiation Protection Association, May 14–19, 2000, JP (T. Ishiguchi, S. Iwanami, S. Kawatsu, T. Ishigaki, S. Koga, Eds.) pp. 1–10. Hiroshima: International Radiation Protection Association. [Google Scholar]
- Jobe AH, Bancalari E. 2001. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 163(7): 1723–1729. [CrossRef] [PubMed] [Google Scholar]
- Kim Y, Choi J, Kim S, Lee C, Cho P, Lee Y, Kim C. 2005. A study on the utilization of diagnostic equipments and patient dose for diagnostic radiological procedures in Korea. Korean J. Med. Phys. 16(1): 10–15. [Google Scholar]
- Lee MC, Lloyd J, Solomito MJ. 2017. Poor utility of gonadal shielding for pediatric pelvic radiographs. Orthopedics 40(4): e623–e627. [CrossRef] [PubMed] [Google Scholar]
- Manuck TA, Rice MM, Bailit JL, Grobman WA, Reddy UM, Wapner RJ, Thorp JM, Caritis SN, Prasad M, Tita AT, Saade GR, Sorokin Y, Rouse DJ, Blackwell SC, Tolosa JE. 2016. Preterm neonatal morbidity and mortality by gestational age: a contemporary cohort. Am. J. Obstet. Gynecol. 215(1): 103.e101–103.e114. [Google Scholar]
- McCarty M, Waugh R, McCallum H, Montgomery RJ, Aszkenasy OM. 2001. Paediatric pelvic imaging: improvement in gonad shield placement by multidisciplinary audit. Pediatr. Radiol. 31 (9): 646–649. [CrossRef] [PubMed] [Google Scholar]
- Ono K, Hada M, Mitarai T, Kato Y, Akahane K, Kai M, Kusama T. 2000. Frequency of X-ray examinations of neonates classified according to their birth weight in NICU. In: International congress of the International Radiation Protection Association, May 14–19, 2000 (K. Ono, M. Hada, T. Mitarai, Y. Kato, K. Akahane, M. Kai, T. Kusama, Eds.) p. 20. Hiroshima, JP: International Radiation Protection Association. [Google Scholar]
- Ono K, Akahane K, Aota T, Hada M, Takano Y, Kai M, Kusama T. 2003. Neonatal doses from X ray examinations by birth weight in a neonatal intensive care unit. Radiat. Prot. Dosimetry 103(2): 155–162. [CrossRef] [PubMed] [Google Scholar]
- Porto L, Lunelli N, Paschuk S, Oliveira A, Ferreira JL, Schelin H, Miguel C, Denyak V, Kmiecik C, Tilly J, Khoury H. 2014. Evaluation of entrance surface air kerma in pediatric chest radiography. Radiat Phys. Chem.104: 252–259. [Google Scholar]
- Puch-Kapst K, Juran R, Stoever B, Wauer RR. 2009. Radiation exposure in 212 very low and extremely low birth weight infants. Pediatrics 124(6): 1556–1564. [CrossRef] [PubMed] [Google Scholar]
- Scott MV, Fujii AM, Behrman RH, Dillon JE. 2014. Diagnostic ionizing radiation exposure in premature patients. J. Perinatol. 34(5): 392–395. [CrossRef] [PubMed] [Google Scholar]
- Smans K. 2009. The development of dose optimisation strategies for X-ray examinations of newborns. Leuven, BE: Katholieke Universiteit Leuven. [Google Scholar]
- Soboleski D, Theriault C, Acker A, Dagnone V, Manson D. 2006. Unnecessary irradiation to non-thoracic structures during pediatric chest radiography. Pediatr. Radiol. 36(1): 22–25. [CrossRef] [PubMed] [Google Scholar]
- Statistics Korea. 2016. Birth statistics 2015. Daejeon: Statistics Korea. [Google Scholar]
- Sung HJ, Han JB, Song JN, Choi NG. 2016. Entrance surface dose according to dose calculation: head and wrist. J. Radiol. Sci. Technol. 39(3): 305–312. [CrossRef] [Google Scholar]
- Sutton PM, Arthur RJ, Taylor C, Stringer MD. 1998. Ionising radiation from diagnostic x rays in very low birthweight babies. Arch. Dis. Child. Fetal Neonatal Ed. 78(3): F227–F229. [Google Scholar]
- United Nations Scientific Committee on the Effects of Atomic Radiation. 2000. Sources and effects of ionizing radiation. UNSCEAR 2000 report to the General Assembly, with scientific annexes. New York, NY: United Nations. [Google Scholar]
- Vachharajani A, Vachharajani NA, Najaf T. 2013. Neonatal radiation exposure. NeoReveiws 14(4): e190. [CrossRef] [Google Scholar]
- Yu CC. 2010. Radiation safety in the neonatal intensive care unit: too little or too much concern? Pediatr. Neonatol. 51(6): 311–319. [Google Scholar]
Cite this article as: Park MJ, Kim SS, Park GY, Hong HS. 2018. Radiation exposure of very-low-birth-weight infants in neonatal intensive care units in Korea. Radioprotection 53(4): 279–286
All Tables
Baseline characteristics of patients grouped by birth weight (≤ 750 g, 751 to ≤ 1000 g, 1001 to ≤ 1250 g, 1251 to ≤ 1500 g).
All Figures
|
Fig. 1 Study flow. LOS: length of stay. |
| In the text | |
|
Fig. 2 Distributions of radiographs in each birth weight group. |
| In the text | |
|
Fig. 3 Entrance skin dose for each birth weight groups. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.