")
")
| Issue |
Radioprotection
Volume 61, Number 2, Avril-Juin 2026
|
|
|---|---|---|
| Page(s) | 146 - 155 | |
| DOI | https://doi.org/10.1051/radiopro/2025035 | |
| Published online | 15 juin 2026 | |
Article
Radiation protection management for the deceased patients in nuclear medicine. Part 1: staff in charge of body transport and embalming
Autorité de Sûreté Nucléaire et de Radioprotection (ASNR), F-92260, Fontenay-aux-Roses, France
* Corresponding author: Cette adresse e-mail est protégée contre les robots spammeurs. Vous devez activer le JavaScript pour la visualiser.
Received:
14
March
2025
Accepted:
7
September
2025
Abstract
In France, in 2007 and 2008, a few deaths occurred for patients who had recently undergone nuclear medicine treatments. Following these events, since there were few guidelines, the French Institute for Radiation Protection and Nuclear Safety (IRSN) investigated radiation protection measures applicable after the death of such patients. An initial study conducted between 2008 and 2016 was updated in 2022 to account for new clinically introduced radionuclides. This article consolidates these efforts to provide a comprehensive overview of operational guidelines for professionals involved in the body transport and embalming of deceased patients after a nuclear medicine treatment. Dose assessments were performed using conservative assumptions based on insights from funeral service professionals. As a result, post-mortem waiting periods required to meet a dose constraint of 300 μSv per operation were established. Except for iodine-131 used in cancer treatment (Sodium iodide, MIBG, and Lipiocis®) and therapeutic indium-111 pentetreotide, the recommended waiting periods were estimated to be less than a week. These recommendations will serve as a valuable resource for nuclear medicine departments and funeral professionals to manage the death of a patient after nuclear medicine treatment.
Key words: radioactive corpse / nuclear medicine / radiation protection / body transport / embalming
© C. Michel et al., Published by EDP Sciences 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
1 Introduction
In France, in 2007 and 2008, a few deaths occurred for patients who had recently undergone nuclear medicine treatments, due to unexpected circumstances and not associated to their treatment nor their disease. Two cases were identified as significant from a radiation protection perspective: the patients died from heart attack less than 24 h after administration: one following iodine-131 MIBG (metaiodobenzylguanidine) treatment (Djoumessi et al., 2009), and the other after treatment with samarium-153 lexidronam pentasodium (Quadramet®) (Lortal et al., 2009). Following these events, the French Institute for Radiation Protection and Nuclear Safety (IRSN) investigated radiation protection measures to implement after the death of patients who underwent nuclear medicine treatments.
Over the period 2008–2016, IRSN conducted an initial study (IRSN, 2017) on radiation exposure risks for professionals involved in transport of deceased patients, and in their embalming. More recently, in 2022, the French Nuclear Safety Authority (ASN) requested IRSN to update the previous assessments including the new clinically introduced radionuclides (IRSN, 2023).
Although early death of patients following nuclear medicine treatment is rare, there is a lack of consensual recommendations to manage such cases. This is highlighted in reports published by the European Commission (European Commission, 1998), the International Commission on Radiological Protection (ICRP Publication 94, 2004), and the International Atomic Energy Agency (IAEA, 2009). Furthermore, to date, no other studies than that of Djoumessi (Djoumessi et al., 2009) have been identified in the literature that assess the radiation exposure of professionals involved in the transport and embalming of deceased patients after nuclear medicine treatments.
Therefore, the aim of this article is to provide a comprehensive overview of practical recommendations from IRSN studies dealing with the occupational radiation protection for the transport and embalming of deceased patients. This includes the main radionuclides used in nuclear medicine as well as the newly ones introduced clinically. A separate study focusing on the exposure of crematorium staff handling radioactive deceased patients has also been conducted and will be presented in a forthcoming publication (Michel et al, accepted).
Overall, this work may be used as a practical guidance for nuclear medicine professionals, hospital mortuary staff, funeral service providers and other stakeholders involved in the management of deceased nuclear medicine patients, if they face this rare situation.
2 Material and methods
2.1 Assumptions, scenarios, and radionuclides considered
The initial IRSN study conducted over the period 2008–2016 was carried out within the framework of an ASN’s working group on deceased patients. Based on the contribution of funeral service professionals participating in this group, dose assessments were performed for two key post-mortem procedures:
Transport of deceased patients: the considered transport corresponds to the first transfer of the patient directly after death and before placing the body into the coffin;
Embalming, including body cleansing, dressing, and thanatopraxy when required.
According to the recommendations of the funeral service professionals involved, the following conservative assumptions were applied for the post-mortem procedures:
The distance from professional to patient body was set at 50 cm for both procedures;
Contact duration was estimated at 1 h for body transport and 2 h for embalming.
The following therapeutic radionuclides were considered:
Beta emitters: phosphorus-32, strontium-89, yttrium-90, indium-111, iodine-131, samarium-153, holmium-166, erbium-169, lutetium-177, and rhenium-186;
Alpha emitters: radium-223 and actinium-225.
Conversely, diagnostic radionuclides were excluded from this assessment, as their external dose rates are significantly lower than those of therapeutic radionuclides due to their shorter half-lives and lower administered activities.
Table 1 summarizes the key characteristics of the considered radionuclides, including half-life, physical or pharmaceutical form, medical application, and administered activities based on clinical practice.
Although some radiopharmaceuticals are no longer in use in France, i.e., phosphorus-32, therapeutic indium-111 pentetreotide, and iodine-131 Lipiodol®, they were included in the analysis given their continued or potential future use in other countries or their possible reintroduction in France.
In this study, external and internal contamination were not considered, assuming that the professionals handling deceased patients use the standard personal protective equipment (e.g., gloves).
Radionuclides considered in this study: physical half-life, physical or pharmaceutical form, medical application, and administered activity.
2.2 Equivalent dose rate coefficients
2.2.1 General case for the radionuclides
In general, equivalent dose rate coefficients were measured from living or deceased individuals, reported in the literature (Abuqbeitah et al., 2018; BIR, 1999; CSHPF, 2006; Dauer et al., 2014; European Commission, 1998; Gardin, 2002; Parlak et al., 2015; Prince et al., 2014; Serencsits et al., 2022).
When measurements were not available, the coefficients were taken from the French technical leaflets “Radioprotection : Radionucléides” jointly published by INRS (French National Institute for Research and Safety) and IRSN (INRS-IRSN, 2013).
The equivalent dose rate coefficients for radionuclides in this case are summarized in Table 2.
Equivalent dose rate coefficients for radionuclides in the general case, excluding pure beta emitters or those with maximum beta energy above 1 MeV.
2.2.2 Specific case: beta emitters (pure or with high beta energy)
For pure beta emitters or radionuclides with a high beta energy, defined here as a maximum beta energy exceeding 1 MeV, the equivalent dose rates from bremsstrahlung radiation were estimated using an envelope approach as described in this section. The yttrium-90 was selected as reference radionuclide because of the extensive data available. For other radionuclides, the coefficients were estimated by applying a linear scaling based on the maximum beta energy.
In a first step, a literature review was conducted for yttrium-90 to identify the highest reported equivalent dose rate coefficient among its three forms: liquid solution, TheraSphere® and SIR-Sphere® (Aubert et al., 2002; McCann et al., 2012).
In a second step, due to lack of data for the other radionuclides and no validated method exists for assessing bremsstrahlung-related equivalent dose rates, values were extrapolated from yttrium-90, by applying a linear scaling with maximum energy of beta. This approach is recognized to overestimate the equivalent dose rate.
In a third step, a distinction was made between radiopharmaceuticals fixed to soft tissues and those fixed to bones. Since bremsstrahlung yield is proportional to the medium’s atomic number, a factor of 21/7.9, representing the ratio of the effective atomic numbers of bone to soft tissue, was applied to the soft-tissue equivalent dose rate to obtain the corresponding value for bone.
The equivalent dose rate coefficients for radionuclides in this case are summarized in Table 3.
Equivalent dose rate coefficients for pure beta emitters and radionuclides with maximum beta energy above 1 MeV.
2.3 Effective half-lives
Effective half-life values were obtained from the literature (see references in Tab. 4). When the data were not available, the physical half-life was used. This choice is conservative, because the biological half-life of radionuclides used in nuclear medicine is generally shorter than the physical half-life. The effective half-lives are summarized in Table 4.
Effective half-lives of radionuclides considered in this study.
2.4 Calculation method
To estimate the effective dose E, the equivalent dose H*(10) at a distance d from the deceased patient over a time interval Δt was calculated using the following formula:
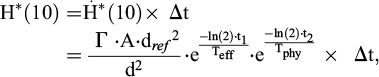 (1)
(1)
where:
 : equivalent dose rate (μSv.h−1);
: equivalent dose rate (μSv.h−1);A: administered activity (GBq);
d: distance from the deceased patient, fixed at 0.5 m for the two post-mortem procedures considered (body transport and embalming);
dref: reference distance, set at 1 m;
Γ: equivalent dose rate coefficient for the considered radionuclide (μSv.h−1.GBq−1);
Teff: effective half-life of the radiopharmaceutical (days);
Tphy: physical half-life of the radionuclide (days);
t1: time between radiopharmaceutical administration and patient death (days);
t2: time between patient death and post-mortem procedure (days).
The equivalent dose rate reflecting the remaining body activity decreases:
according to the effective half-life, due to biological excretion and physical decay, between radiopharmaceutical administration and patient death
according to the physical half-life, after the patient death.
Applying this approach leads to intentionally overestimated effective doses, for the following reasons:
the equivalent dose rate at 0.5 m was derived from the equivalent dose rate at 1 m value using the inverse square law which applies strictly to a point source;
the assumption of continuous presence of the professional at 0.5 m;
the selection of highest values as reported in the literature for equivalent dose rate coefficients and effective half-lives.
2.5 Dose criterion
Professionals involved in body transport or in embalming are workers who are not classified for radiation protection purposes. In France, regulation requires that the risk assessment demonstrating the effective dose likely to be received by these workers remains below 1 mSv per year for them to remain unclassified (JORF, 2023).
To ensure compliance with this limit and given that exposure situations for these workers are difficult to control because of their rarity, IRSN adopted a dose criterion below this value, corresponding to one-third (rounded to the nearest 100 µSv), i.e., 300 µSv per post-mortem procedure. In the even rarer scenario of a funeral professional handling three deceased patients in the same year, a dose of 300 μSv per operation would still result in a total annual dose below 1 mSv. For the longest operation (i.e., embalming which lasts 2 h) the 300 μSv criterion is met if the dose rate at the working distance of 0.5 m is below 150 μSv/h.
This approach allocating only a fraction of the 1 mSv limit has been used previously, for example in the European Commission’s Radiation Protection 97 report (European Commission, 1998) on public exposure from iodine-131 patients. This fraction ensures compliance with the 1 mSv limit even if the public is exposed to other artificial sources during the year.
Ideally, to justify the selection of dose criterion value, it would be necessary to assess the annual number of early deaths after nuclear medicine treatment. In fact, this information is not systematically reported to the related authority since it is not considered as a significant event in radiation protection. The only relevant data was published by the Federal Agency for Nuclear Control for crematorium staff (FANC, 2011). Dose rate measurements were performed on more than 3,380 deceased individuals over a six-month period in a Belgian crematorium. Dose rates above background radiation (threshold) were detected in approximately 1 out of 500 deceased individuals. In fact, the positive cases corresponded to patients who underwent diagnostic nuclear medicine procedures and not therapeutic ones. These findings confirm that the early deaths after nuclear medicine treatment are very rare.
We considered that these results observed in the studied Belgian cohort could be generalized and applied in France. Therefore, we considered that the early deaths after nuclear medicine treatment are also very rare. This is also confirmed by the only two French cases occurred in 2007 and 2008 mentioned above. Consequently, the adoption of a 300 μSv criterion was deemed an appropriate and conservative hypothesis assuming three cases could occur per year and managed by the same funeral professional. This leads to meeting the annual limit of 1 mSv.
This 300 µSv criterion was used to calculate the waiting periods required before handling the deceased patient, based on the doses likely to be received by workers using Equation #1.
More specifically, when it is not possible to manage the deceased patient immediately because the dose would exceed the criterion, two types of periods were calculated:
If the death occurs at the time of radiopharmaceutical administration (worst case for radiation protection), a minimum waiting period after death is calculated. Using Equation #1, this case corresponds to t1=0, and then t2 corresponding to the waiting period is calculated.
Otherwise, the minimum time interval between radiopharmaceutical administration and death that allows for immediate management of the deceased patient, is calculated. Using Equation #1, this case corresponds to t2=0, and then t1 corresponding to this time interval is calculated.
3 Results
Based on the calculated doses for body transport and embalming, and with respect to the 300 μSv dose criterion, two scenarios can be distinguished. Either the deceased patient can be managed immediately after death, or a waiting period is required before transport and/or embalming.
3.1 Immediate management of the deceased patient
This scenario corresponds to a dose rate below 150 μSv/h at 0.5 m from the deceased patient at the time of death, as explained above. The procedures include:
Phosphorus-32 for polycythemia treatment;
Strontium-89 for palliative treatment of bone metastases;
Yttrium-90 for treatment of non-Hodgkin’s lymphoma with ibritumomab tiuxetan, treatment of liver cancers using microspheres, and radiation synovectomy;
Iodine-131 for non-cancer thyroid treatment with administered activity below 700 MBq;
Erbium-169 and rhenium-186 for radiation synovectomy;
Radium-223 for palliative treatment of bone metastases;
Actinium-225 for treatment of metastatic prostate cancer targeting PSMA (prostate-specific membrane antigen).
3.2 Waiting periods required between death and post-mortem procedure
The procedures include:
Indium-111 for treatment of tumors expressing somatostatin receptors;
Iodine-131 for non-cancer thyroid treatment with an administered activity between 700 and 800 MBq, and for treatment of thyroid cancer;
Samarium-153 for palliative treatment of bone metastases;
Holmium-166 for treatment of liver cancers using microspheres;
Lutetium-177 for treatment of intestine tumors with DOTATATE (Lutathera®) and for treatment of metastatic prostate cancer targeting PSMA.
3.2.1 Death immediately following radiopharmaceutical administration
The minimum waiting periods after death when death occurs immediately following administration (worst case for radiation protection) are summarized in Table 5.
According to French regulations (JORF, 2011), at the time of the study, body transport had to be completed within 48 h after death, and embalming within 6 days. For radiation protection reasons, these time limits might need to be exceeded for indium-111-pentetreotide, iodine-131 for thyroid cancer, iodine-131-MIBG, and iodine-131-lipiocis®. In such cases, an exemption had to be granted by the State representative to exceed the legal time limits. However, in 2024, French regulations were modified (JORF, 2024), and embalming must now be performed within 14 days. Therefore, the number of cases requiring exemptions is slightly reduced and now limited to those of indium-111-pentetreotide (transport only), iodine-131 for thyroid cancer (3.7 and 5.6 GBq administered), iodine-131-MIBG and iodine-131-Lipiocis (transport only).
Calculated waiting periods from time of death to body transport and embalming meeting the 300 μSv dose criterion per post-mortem procedure, for the scenario of death immediately following radiopharmaceutical administration (worst case for radiation protection).
3.2.2 Death some days after radiopharmaceutical administration
If death does not occur immediately after administration, it is possible to calculate the minimum time interval between administration and death that allows the deceased patient to be managed immediately after death.
These time intervals are summarized in Table 6.
Calculated time intervals between administration and death allowing immediate body transport and embalming, meeting the 300 μSv dose criterion per post-mortem procedure.
3.3 Hospitalization of patients: Death after patient release
For certain treatments in France, patients are systematically hospitalized. In most French nuclear medicine departments, the equivalent dose rate is measured at the time of patient release, with a release criterion generally set at 20–25 μSv/h at 1 meter from the patient. If the release criterion is met at patient release and if the patient dies afterwards, the equivalent dose criterion of 150 μSv/h is inherently satisfied. Therefore, the deceased patient can be transported and embalmed immediately.
3.4 Synthesis of recommendations
The recommendations for all radiopharmaceuticals considered in this study are summarized in Table 7 for therapeutic procedures requiring no special radiation protection measures and Table 8 for others.
Therapeutic procedures for which no special radiation protection measures are required for transport and embalming of deceased patients, meeting the 300 μSv dose criterion per post-mortem procedure.
Therapeutic procedures and administered activities requiring radiation protection measures for transport and embalming of deceased patients. Waiting periods under 1 day are shown in hours (rounded up) and those over 1 day in days (rounded up).
4 Discussion
The results of this study indicate that the radiation protection following a patient’s death can be effectively addressed through recommendations based on estimated exposures of workers handling the deceased patient.
For lutetium-177, radium-223, actinium-225 and holmium-166 considered as the most recently introduced therapeutic radionuclides in France, the calculated waiting periods between patient death and transport or embalming, meeting the dose criterion, were under 6 days. This result matches the embalming time limit in France at the time of the calculations (2022).
More recently, since 2024, the regulations have changed (JORF, 2024) and the time limit for embalming has been extended to 14 days. Consequently, regardless of whether the limit is 6 or 14 days, no exemption from State representatives is required for the 4 new radionuclides listed above.
In some other countries, radiation protection recommendations differ from those in France, for example in Belgium (FANC, 2025) and Switzerland (DFI-IFSN, 2017). They are not based on exposure estimates, but on exemption levels of radioactivity.
In Belgium, an Excel-based calculator is available (FANC, 2025) to calculate a precaution period according to the radiopharmaceutical and the administered activity. This period is related to the radiological risks. In other terms, if a patient dies within this period which start from radiopharmaceutical administration, special radiation protection precautions are needed to manage the deceased patient. These precautions are based on radiation protection principles (time, distance, shielding), and hygiene rules to avoid contamination. Regardless of the level or type of radioactivity present, thanatopraxy is prohibited in Belgium.
Because the underlying concepts differ between France and Belgium, the Belgian precaution period is not directly comparable to the two types of time frame calculated for France, namely the waiting period after death and the time interval between administration and death.
However, it is possible to show, in these two countries, the practical consequences for the example of administration of 7.4 GBq of lutetium-177-PSMA:
In the first case, in France according to this study, if the death occurs immediately after administration, the deceased patient can be transported immediately without specific radiation protection precautions, while a waiting period of 4 days is necessary to embalm (body cleansing, dressing, and thanatopraxy). In Belgium, the precaution period is 28 days, and then precaution measures must be taken for body transport, body cleansing and dressing, based on basic principles of radiation protection (time, distance, shielding) and hygiene to avoid contamination.
In the second case, if the death occurs 1 week after administration, no specific radiation protection precautions are necessary for body transport and embalming in France according to this study. In Belgium, the time of death is still within the precaution period of 28 days, therefore the same precautions as in the first case have to be followed.
In the third case, if the death occurs 1 month after administration, no specific radiation protection precautions are necessary for body transport and embalming (body cleansing, dressing and thanatopraxy) in France according to this study. In Belgium, since the death occurs after the precaution period of 28 days, no specific radiation precautions are necessary for body transport, body cleansing and dressing.
In France, if a patient who has recently undergone nuclear medicine treatment dies in the same healthcare facility, the healthcare professionals are generally aware of the recent treatment. In such cases, radiation protection measures can be implemented, with the assistance of radiation protection staff, if needed. For example, active or passive dosimeters can be worn by staff, and radiation exposure can be minimized by applying the standard rules of time, distance and shielding, and hygiene rules to avoid contamination. A recommended practice is to follow pre-established written internal procedures. Furthermore, depending on the circumstances, the funeral professionals may be informed by the healthcare facility. However, there is no legal obligation to inform them of the radioactive status of the deceased patient, as death certificate does not include a section for this information.
If a patient dies at home after a nuclear medicine treatment, it is more likely that the funeral professionals will not be aware of the recent treatment, as the only way for them to know is to be informed by the deceased patient’s next of kin.
To mitigate this potential lack of information, patients could be advised to carry a release card at all times for a certain period after the treatment. This card would specify the received treatment and provide the contact details of the nuclear medicine department. Such a card has been developed by HERCA (Heads of the European Radiological Protection Competent Authorities) (HERCA, 2012). Using the HERCA model, a release card has been implemented in Belgium since 2020. (FANC, 2020).
5 Conclusion
This study was based on calculations using conservative assumptions. The study assessed the scenarios in which post-mortem procedures (transport and embalming) could be performed on deceased patients after nuclear medicine treatment, while ensuring that the effective dose to the workers remains below 300 µSv per operation.
For each common type of nuclear medicine treatment, practical recommendations were proposed for nuclear medicine departments and funeral professionals in the event of a patient death. This considers the administered radiopharmaceutical and its activity, the time interval between administration and death, as well as the dose rate around the deceased patient, if applicable.
For most nuclear medicine treatments, no special radiation protection measures are required, even if the death occurs immediately after administration of the radiopharmaceutical. However, some radiopharmaceuticals require a more precautionary approach, involving waiting periods before transport and embalming. For the most recent therapeutic radionuclides as lutetium-177, radium-223, holmium-166, and actinium-225 the waiting periods are under one week and fall within the legal time limits in France.
Acknowledgments
The authors thank the professionals at the French cancer center visited following the death of a patient who benefited from a technetium-99m procedure, in particular the members of the radiation protection department and those involved in the management of deceased patients (mortuary chamber officers and their manager).
The authors also thank the professionals at the French university hospital visited following the death of a patient treated with lutetium-177.
Funding
This work was carried out within the framework of a referral from the French Nuclear Safety Authority (ASN) to the French Institute for Radiation Protection and Nuclear Safety (IRSN) in April 2020.
Conflicts of interest
The authors declare that they have no conflict of interest.
Data availability statement
The research data associated with this article are included within the article.
Author contribution statement
All authors contributed to the work related in this article, and all reviewed and approved the final version of the manuscript.
Ethics approval
Ethical approval was not required.
Informed consent
This article does not contain any studies involving human subjects.
References
- Abuqbeitah M, Demir M, Uslu-Beşli L, Yeyin N, Sönmezoğlu K. 2018. Blood clearance and occupational exposure for 177Lu-DOTATATE compared to 177Lu-PSMA radionuclide therapy. Radiat Environ Biophys 57: 55–61. [Google Scholar]
- Aubert B, Guilabert N, Lamon A, Ricard M. 2002. Aspects de radioprotection liés à de nouveaux protocoles de radiothérapie interne par l’yttrium 90. https://sfrp.asso.fr/wp-content/uploads/2021/11/30-aubert.pdf [Google Scholar]
- BIR. 1999. Patients leaving hospital after administration of radioactive substances. Working Party of the Radiation Protection Committee of the British Institute of Radiology. Br J Radiol 72: 121–125. [Google Scholar]
- Calais PJ, Turner JH. 2014. Radiation safety of outpatient 177Lu-octreotate radiopeptide therapy of neuroendocrine tumors. Ann Nucl Med 28: 531–539. [Google Scholar]
- CIS bio international. 2006. Summary of Product Characteristics - LIPIOCIS. [Google Scholar]
- CIS bio international. 2017. Summary of Product Characteristics − IOBENGUANE [131 I] Pour Thérapie. [Google Scholar]
- CSHPF. 2006. Précautions recommandées aux patients ayant bénéficié d’un traitement par l’iode radioactif afin de limiter l’exposition aux rayonnements ionisants des personnes à son contact. [Google Scholar]
- Dauer LT, Williamson MJ, Humm J, O’Donoghue J, Ghani R, Awadallah R, Carrasquillo J, Pandit-Taskar N, Aksnes A-K., Biggin C, Reinton V, Morris M, St Germain J. 2014. Radiation safety considerations for the use of 223RaCl2 DE in men with castration-resistant prostate cancer. Health Phys 106: 494–504. [Google Scholar]
- DFI-IFSN. 2017. Ordonnance du DFI sur l’utilisation des matières radioactives (OURM). Version in force since 1 January 2018. https://www.fedlex.admin.ch/eli/cc/2017/509/fr [Google Scholar]
- Djoumessi CF, Bramoulle C, Prunier C, Baulieu JL, Besnard JC. 2009. Évaluation et gestion du risque radioactif suite au décès d’un patient ayant reçu une dose thérapeutique d’iode-131 dans le cadre d’un traitement en radiothérapie métabolique. Radioprotection 44: 319–328. [Google Scholar]
- European Commission. 1998. Radiation Protection Following Iodine-131 Therapy − Exposures due to Out-patients or Discharged In-patients − Radiation Protection 97. [Google Scholar]
- EMA. 2021. Summary of Product Characteristics − Lutathera. [Google Scholar]
- FANC. 2011. Recommandations pour le personnel des crématoriums en cas de manipulation de dépouilles radioactives. [Google Scholar]
- FANC. 2020. Règlement technique du 29 juin 2020 fixant le modèle de la carte de sortie après l’administration à une personne d’un produit radioactif à des fins radiothérapeutiques. [Google Scholar]
- FANC. 2025. Website of Federal Agency for Nuclear Control (FANC) − Dépouilles radioactives. https://afcn.fgov.be/fr/professionnels/professions-medicales/medecine-nucleaire/initiatives-de-lafcn/depouilles-radioactives. [Google Scholar]
- Gardin I. 2002. Recommandations en radiothérapie métabolique vis à vis de la radioprotection des populations. Médecine Nucl. [Google Scholar]
- HERCA. 2012. HERCA Patient Release Card. https://www.herca.org/herca-patient-release-card/. [Google Scholar]
- IAEA. 2009. Release of Patients After Radionuclide Therapy − Safety Reports Series No. 63. [Google Scholar]
- ICRP Publication 94. 2004. Release of patients after therapy with unsealed radionuclides. Ann ICRP 26. [Google Scholar]
- INRS-IRSN. 2013. Radioprotection : Radionucléides − Indium-111 − ED 4315. https://www.inrs.fr/media.html?refINRS=ED%204315. [Google Scholar]
- IRSN. 2017. Conduite à tenir devant une dépouille humaine après un traitement de médecine nucléaire ou de curiethérapie par implants permanents − Avis IRSN/ 2017-00174. https://www.irsn.fr/sites/default/files/documents/expertise/avis/2017/Avis-IRSN-2017-00174.pdf. [Google Scholar]
- IRSN. 2023. Nouveaux radionucléides en médecine nucléaire − Quatrième partie: Radioprotection des travailleurs prenant en charge les patients décédés après un acte de médecine nucléaire − Rapport IRSN n° 2023-00026. https://www.irsn.fr/sites/default/files/2023-12/Rapport-IRSN-2023-00026.pdf. [Google Scholar]
- Jones JR. 2004. Excretion and Retention in Targeted Radionuclide Therapy − A Presentation of the Results for 7 Radiotherapeutic Modalities. https://www.ipen.br/biblioteca/cd/irpa/2004/files/4d8.pdf. [Google Scholar]
- JORF. 2011. Articles R. 2213-11, R. 2213-33 et R. 2213-35 du code général des collectivités territoriales. Versions in force between 31 January 2011 and 12 July 2024. [Google Scholar]
- JORF. 2023. Article R. 4451-57 du code du travail. Version in force since 23 June 2023. [Google Scholar]
- JORF. 2024. Articles R. 2213-33 et R. 2213-35 du code général des collectivités territoriales. Versions in force since 12 July 2024. [Google Scholar]
- Kurth J, Krause BJ, Schwarzenböck SM, Stegger L, Schäfers M, Rahbar K. 2018. External radiation exposure, excretion, and effective half-life in 177Lu-PSMA-targeted therapies. EJNMMI Res 8: 32. [Google Scholar]
- Lortal B, Caron J, Dejean C, Bonichon F, Houédé N, Buj S, Cazeau A-L. 2009. Gestion du risque radioactif associé au décès d’un patient 12 heures après injection de Quadramet®. Médecine Nucl 33: 754–757. [Google Scholar]
- McCann JW, Larkin AM, Martino LJ, Eschelman DJ, Gonsalves CF, Brown DB. 2012. Radiation emission from patients treated with selective hepatic radioembolization using yttrium-90 microspheres: are contact restrictions necessary? J Vasc Interv Radiol JVIR 23: 661–667. [Google Scholar]
- Parlak Y, Gumuser G, Sayit E. 2015. Samarium-153 therapy for prostate cancer: the evaluation of urine activity, staff exposure and dose rate from patients. Radiat Prot Dosimetry 163: 468–472. [Google Scholar]
- Petyt G, Cougnenc O, Defachelles A-S., Cazin J-L., Carpentier P. 2009. Radioprotection après injection thérapeutique de [131I]-mIBG : données préalables à l’ouverture du protocole MIITOP-0607. Médecine Nucl 33: 729–736. [Google Scholar]
- Prince JF, Smits MLJ, Krijger GC, Zonnenberg BA, van den Bosch MAAJ, Nijsen JFW, Lam MGEH. 2014. Radiation emission from patients treated with holmium-166 radioembolization. J Vasc Interv Radiol JVIR 25: 1956–1963. e 1. [Google Scholar]
- Serencsits B, Chu BP, Pandit-Taskar N, McDevitt MR, Dauer LT. 2022. Radiation Safety Considerations and Clinical Advantages of α-Emitting Therapy Radionuclides. J Nucl Med Technol 50: 10–16. [Google Scholar]
- U.S. NRC. 2020. Release of Patients Administered Radioactive Material. https://www.nrc.gov/docs/ML1923/ML19232A081.pdf. [Google Scholar]
- Venencia CD, Germanier AG, Bustos SR, Giovannini AA, Wyse EP. 2002. Hospital discharge of patients with thyroid carcinoma treated with 131I. J Nucl Med Off Publ Soc Nucl Med 43: 61–65. [Google Scholar]
Cite this article as: Michel C, Célier D, Isambert A. 2026. Radiation protection management for the deceased patients in nuclear medicine. Part 1: staff in charge of body transport and embalming. Radioprotection 61(2): 146–155. https://doi.org/10.1051/radiopro/2025035
All Tables
Radionuclides considered in this study: physical half-life, physical or pharmaceutical form, medical application, and administered activity.
Equivalent dose rate coefficients for radionuclides in the general case, excluding pure beta emitters or those with maximum beta energy above 1 MeV.
Equivalent dose rate coefficients for pure beta emitters and radionuclides with maximum beta energy above 1 MeV.
Calculated waiting periods from time of death to body transport and embalming meeting the 300 μSv dose criterion per post-mortem procedure, for the scenario of death immediately following radiopharmaceutical administration (worst case for radiation protection).
Calculated time intervals between administration and death allowing immediate body transport and embalming, meeting the 300 μSv dose criterion per post-mortem procedure.
Therapeutic procedures for which no special radiation protection measures are required for transport and embalming of deceased patients, meeting the 300 μSv dose criterion per post-mortem procedure.
Therapeutic procedures and administered activities requiring radiation protection measures for transport and embalming of deceased patients. Waiting periods under 1 day are shown in hours (rounded up) and those over 1 day in days (rounded up).
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.