")
")
| Issue |
Radioprotection
Volume 61, Number 1, Janvier-Mars 2026
|
|
|---|---|---|
| Page(s) | 48 - 54 | |
| DOI | https://doi.org/10.1051/radiopro/2025025 | |
| Published online | 20 March 2026 | |
Article
Assessment of the cumulative dose in computed tomography (CT) in Moroccan hospitalized patients
1
Laboratory of Health Sciences, Care and Techniques, Higher Institute of Nursing Professions and Health Techniques, Fez, Morocco
2
Laboratory of Engineering Sciences, Polydisciplinary Faculty of Taza, USMBA, Fez, Morocco
3
Human Pathology, Biomedicine and Environment Laboratory, Faculty of Medicine and Pharmacy, USMBA, Fez, Morocco
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
27
December
2024
Accepted:
24
June
2025
Abstract
An increase in the frequency of CT scan usage has been observed in most countries worldwide in recent years. This growing use raises concerns about the potential long-term risk of radiation-induced cancer. In this context, and in line with ICRP recommendations, the objective of this study is to evaluate the cumulative effective dose in hospitalized patients who underwent multiple CT scans over the course of one year.
We conducted a retrospective study based on the analysis of data from the medical records of 60 hospitalized patients who underwent multiple CT scans over a one-year period in a Moroccan radiology center.
Regarding the distribution of the annual cumulative effective dose per patient in our sample, the average value was approximately 40 mSv, while the 75th percentile reached 50.7 mSv. Patients who received a dose exceeding 100 mSv per year accounted for 1.6% of our total sample, while 26.6% of patients received a cumulative effective dose between 50 mSv and 100 mSv.
The analysis of our results underscores the importance of strengthening the principles of justification for radiological examinations and dose optimization to enhance patient safety and ensure a more responsible use of ionizing radiation in medical settings.
Key words: Computed tomography / effective doses / stochastic effects / dose optimization
© A. Housni et al., Published by EDP Sciences 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
1 Introduction
Generally, on a global scale, the main source of the population’s exposure to artificial ionizing radiation comes from medical procedures, primarily for diagnostic purposes. Among these procedures, CT scans hold a predominant position (IRSN, 2020a; Dreuil and Etard, 2017; Karim et al., 2016). Their increasingly frequent use raises the question of the potential long-term risk of radiation-induced cancer, especially since the dose delivered during CT examinations is significantly higher than that received in conventional radiology, while their frequency of use continues to rise (Alashban et al., 2023; Bourguignon, 2021, Smith-Bindman et al., 2019).
Although opinions on the long-term effects of low radiation doses remain controversial, the risk cannot be excluded and increases with the dose received due to the cumulative effect of radiation, which, once absorbed, is never neutralized. The risk is therefore heightened by repeated exposures. At a certain level of cumulative energy deposited by radiation, this energy can damage DNA and may potentially contribute to the development of pathology, although other factors may also play a role in cancer development (Dubousset et al., 2016).
Several studies show an increased risk of cancer depending on the dose delivered during CT scan examinations (Shubayr et al., 2023). Additionally, the BEIR VII report (Biological Effects of Ionizing Radiation) estimates that approximately one in 200 people would develop a fatal cancer after an exposure of 100 mSv (Venneri et al., 2009). Other studies have estimated that 1.5% to 2% of cancers diagnosed annually in the United States are associated with CT scan exposure (Brenner et al., 2007; Berrington et al., 2009). In this context, and for radiological protection purposes, it is scientifically plausible to assume that the incidence of carcinogenic or hereditary effects increases proportionally with the equivalent dose received by the affected organs and tissues (ICRP, 2007).
Stochastic effects include radiation-induced cancers and hereditary effects, and they are predominant at low doses. It is widely accepted that there is no threshold dose for their occurrence. Their probability of occurrence increases with the dose according to a dose-response relationship, which can be complex (Laurier et al., 2017). Their severity is independent of the exposure level but depends on the type of pathology and its stage of development at the time of diagnosis.
The goal of patient radioprotection in medical imaging is to prevent harmful effects attributable to ionizing radiation. To assess these effects, the concept of effective dose (E) was introduced by the ICRP in Publication 60 (ICRP, 1991). This concept reflects the potential biological effect induced by ionizing radiation exposure on the organs and tissues of the entire body. The effective dose (E) represents the impact of the absorbed dose in terms of risk to the entire body. It is particularly useful when summing the risks from different exposures received successively by the same individual. The calculation of the cumulative effective dose for our sample was based on the recommendations of ICRP 103 (ICRP, 2007).
At Morocco, in the absence of legally regulated national diagnostic reference levels (DRLs), studies are being conducted to assess professional practices in computed tomography by recording the radiation doses delivered to adult patients. The objective is to establish local diagnosticreference levels and compare them with internationally published DRLs (Benamar et al., 2023; El Mansouri et al., 2022). However, to our knowledge, no Moroccan study has addressed the issue that may arise from the repetition of CT scans over a short period, particularly among hospitalized patients.
However, it is estimated that 20% to 77% of CT scan procedures are unnecessary (Oikarinen et al., 2009). In daily practice, hospitalized patients often undergo more than one CT scan for various reasons: cancer staging, monitoring disease progression, confirming interpretations, evaluating chemotherapy responses, guiding biopsies, or visualizing volume changes. Moreover, X-ray CT scan is the most irradiating medical examination, with ionizing radiation doses approximately 10 times higher than conventional X-rays.
The repetition of CT scans in hospitalized patients leads to a significant accumulation of doses over a short period. This accumulation can have adverse effects, highlighting the need to assess the impact of cumulative doses in a hospital setting. In this context, and in line with ICRP recommendations, the objective of this work is to assess the cumulative effective dose in hospitalized patients who have undergone multiple CT scans over the course of one year. Furthermore, this study aims to assess the need to optimize CT scan protocols and establish a structured approach to improving practices. This involves paying particular attention to radiation protection principles, namely the justification and optimization of the dose delivered to the patient. It also seeks to raise awareness among prescribers, radiologists, and technologists about the administered and cumulative doses resulting from successive examinations.
2 Materials and methods
We conducted a retrospective study based on the analysis of data from the medical records of hospitalized patients who underwent one or more CT scans over a one-year period, from June 12, 2022, to June 11, 2023, in a Moroccan radiology center that receives a large number of both outpatient and hospitalized patients.
2.1 Materials
All examinations were performed using a REVOLUTION EVO scanner from General Electric, equipped with 64 detector rows and 128 slices, featuring Highlight Carety detector technology. The tube had a Performix 40 Plus power type with a dual Focalspot function and a rotation speed of 0.35 s. The collimation was set to 1.25 × 16, and the acquisition mode was helical. The scans were conducted according to predefined standard protocols, with the only adjustable parameter being the acquisition length tailored to the patient’s size. The voltage was set to 120 kV for chest, abdominal, and chest-abdomen-pelvis examinations, except for brain exams where the voltage was set to 140 kV. The load was automatically modulated by an integrated software, ASIR V.
2.2 Sample
Our sample consisted of 60 hospitalized patients who underwent multiple CT scans using identical or different protocols among the most commonly applied. Patients were selected based on the following inclusion and exclusion criteria:
2.2.1 Inclusion criteria
Hospitalized patients who underwent multiple CT scans within a time interval of one year or less, between June 12, 2022, and June 11, 2023.
2.2.2 Exclusion criteria
Hospitalized patients who underwent only one CT scan;
Hospitalized patients who underwent multiple CT scans with a time interval greater than one year;
Hospitalized patients with incomplete medical records.
2.3 Data collection and analysis
Data were collected using an observation grid, recording the examination dates as well as variables such as the age and gender of patients from their medical records. Information on dosimetric indicators, specifically CTDIvol (Computed Tomography Dose Index volume) and DLP (Dose-Length Product), was manually retrieved from the dosimetric reports generated post-acquisition and stored on the PACS (Picture Archiving and Communication System). For each acquisition and the entire examination, the CTDIvol and DLP values were documented.
The effective dose E, expressed in millisieverts (mSv), was estimated by multiplying the DLP (in mGy · cm) by the conversion factors Epdl defined in the International Commission on Radiological Protection’s (ICRP) Publication 103 (2007).
The calculation of the cumulative effective dose for our sample was performed using the following formula:

Epdl (mSv.mGy.cm): conversion factors corresponding to the values 0.0021, 0.0148, 1.0154, and 0.015 for different anatomical regions, namely the brain, chest, abdomen, and thoraco-abdomino-pelvic regions, respectively (ICRP, 2007).
DLPtotal (mGy.cm): the sum of the DLP values for the examinations successively performed on the patient over the course of a year
The data are collected from the PACS (Picture Archiving and Communication System) and statistically analyzed using SPSS software, employing the Kolmogorov-Smirnov test.
The right to anonymity, the confidentiality of information, and its fair and equitable processing were all taken into account in accordance with ethical principles.
3 Results
Our study included sixty hospitalized adult patients of both sexes, comprising 35 men (58.33%) and 25 women (41.67%). The average age of the sample was 47 years, with an age range from 20 to 82 years. During the one-year period, patients underwent more than one examination, whether of the same type or different types (Tab. 1).
The analysis of the distribution of the collected dosimetric data is presented by type of examination in terms of averages, standard deviations, and the 25th and 75th percentiles, as well as minimum and maximum values (Tabs. 2–5).
In Tables 2 and 3, the average, minimum, and maximum values of the CTDIvol (Computed Tomography Dose Index volume) per acquisition for cranial, thoracic, abdominal, and thoraco-abdomino-pelvic examinations were respectively 52.13 mGy (23.62–58.47), 9.54 mGy (5.64–13.31), 11.98 mGy (4.86–17.11), and 10.62 mGy (4.79–17.11). Similarly, in Table 3, the average, minimum, and maximum values of the DLP (Dose-Length Product) for these same examinations were respectively 1065.8 mGy · cm (353.81–1987.66), 366.96 mGy · cm (188.87–509.44), 603.54 mGy · cm (103.76–1055.37), and 720.65 mGy · cm (188–1296).
Tables 4 and 5 present the distribution of total CTDIvol and DLP values per patient over one year, categorized by type of examination. The average, minimum, and maximum CTDIvol values were respectively 166.66 mGy (54.75–453.03), 24.53 mGy (13.31–35.09), 47.93 mGy (7.26–144.47), and 33.79 mGy (9.16–68.29) for cranial, thoracic, abdominal, and thoraco-abdomino-pelvic examinations. Regarding the total DLP, the average, minimum, and maximum values were respectively 3381.02 mGy · cm (1087.95–9227.77), 943.61 mGy · cm (509.44–1214.57), 2414.14 mGy · cm (182.1–8251.7), and 2292.98 mGy · cm (680.05–4584.13) for the aforementioned examination types.
Figure 1 illustrates the distribution of the cumulative annual effective dose per patient in our sample. The average value was approximately 40 mSv, while the 75th percentile was 50.7 mSv. Patients who received a dose exceeding 100 mSv per year represented 1.6% of our total sample, whereas 26.6% of patients had a cumulative effective dose between 50 mSv and 100 mSv.
Characteristics of CT scans.
Distribution of the values of the volumetric CT dose index (CTDIvol) (mGy) per acquisition for each CT scan type.
Distribution of the values of the dose length product (DLP) (mGy.cm) per acquisition for each CT scan type.
Distribution of the values of the Volumetric CT dose index (CTDI vol) (mGy) per patient over one year for each CT scan type.
Distribution of the values of the dose length product (DLP) (mGy.cm) per patient over one year for each CT scan type.
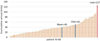 |
Fig. 1 Distribution of the cumulative annual effective dose per patient. |
4 Discussion
The average age of the patients in our sample was 47 years, with extremes ranging from 20 to 82 years. One-third of the patients were under 40 years old, and 50% were under 50 years old, highlighting a significant proportion of young individuals in our sample. This observation emphasizes the importance of protection against the stochastic effects of ionizing radiation for this patient category. Indeed, the International Commission on Radiological Protection (ICRP) confirms that the younger a person is exposed, the higher the risk of radiation-induced cancer (ICRP 2007). Therefore, the principles of justification and dose optimization for each patient, regardless of age or medical history, must remain a priority for all professionals involved in CT scanning.
The 60 patients in our sample underwent 159 examinations, with an average of 2.65 scans per patient and a maximum of 5 scans. Abdominal, thoraco-abdomino-pelvic (TAP), and cranial scans were the most frequent, accounting for 35%, 32.7%, and 27% of the total examinations, respectively.
The 75th percentile values of CTDIvol (mGy) per acquisition in our sample were 56.7, 11.82, 16.1, and 12.32 for cranial, thoracic, abdominal, and TAP protocols, respectively. Similarly, the 75th percentile values of DLP (mGy · cm) were 1166.76, 450, 866.69, and 919.8 for the same protocols. The comparison of these values with published data from other local studies (Tab. 6) revealed that our results were slightly higher for abdominal and chest-abdomen-pelvis examinations. However, the comparison of these values with published data from other countries revealed that our results were higher than the diagnostic reference levels (DRLs) in France (IRSN 2023), Germany (Schegerer et al., 2019), and Australia (Lee et al., 2020) but lower than those adopted in other countries. These significant discrepancies suggest that the principle of dose optimization for patients is not yet well implemented. Indeed, these increases can be attributed to the use of high voltage. Studies on voltage reduction have demonstrated a significant decrease in the delivered dose without compromising the diagnostic quality of images. Furthermore, the high values observed in this study may be explained by the use of higher mAs for each CT examination, as well as by long acquisition lengths. Additionally, the dose can vary significantly when collimation decreases, which could also contribute to the increase in local values.
The repetition of CT scans with an increased number of acquisitions over one year leads to very high DLP values, as shown in Table 4. These results corroborate those of another Moroccan study conducted on cancer patients undergoing multiple CT/TAP scans for cancer staging, with cumulative total DLP values reaching up to 3500 mGy · cm as a maximum and 2012.8 mGy · cm as an average (Bougana et al., 2018).
Analysis of our study results showed that patients received significant cumulative effective doses over one year, with an average value of 40 mSv, a 75th percentile of 50.7 mSv, and a maximum value of 127 mSv. 1.6% of the patients received a dose exceeding 100 mSv per year, a small but significant percentage, while 26.6% accumulated an effective dose between 50 mSv and 100 mSv. Thus, the repetition of CT scans could push the cumulative dose beyond 100 mSv, a threshold considered the upper limit of low doses. Beyond this value, probabilistic effects may be masked by deterministic effects, with an increased probability of deterministic effects and a significant risk of cancer. The ICRP considers 100 mSv as the maximum value for a reference level. Exposures exceeding this reference should only be justified in exceptional or unavoidable circumstances (ICRP 2007).
Studies indicate that patients receiving doses above 100 mSv from CT scans are not uncommon. A review by “Euro Safe” of the European Society of Radiology reported that cumulative effective doses from repeated CT scans could exceed 100 mSv in a small number of patients (approximately 0.5%), most of whom are cancer patients (Frija et al., 2021). Moreover, a large retrospective study conducted across 279 hospitals from January 2015 to December 2019, examining doses received in a single day, showed that 9.4% of patients underwent more than one CT scan, 0.03% received a dose exceeding 100 mSv, and 0.8% received a dose exceeding 50 mSv in a single day (Rehani et al., 2021, Bourguignon, 2021).
Most studies assessing the effects of ionizing radiation on patients are based on survivors of Hiroshima and Nagasaki to estimate the cancer risk from low-dose exposure. Analysis of this cohort revealed an excess of leukemia from five years after exposure and an excess of solid cancers after ten years (Little, 2009).
In our sample, 1.6% of the patients received doses above 100 mSv, and 26.6% received doses between 50 and 100 mSv, indicating an increased cancer risk. Epidemiological data suggest that the threshold for excess cancer incidence lies between 10 and 50 mSv for acute exposure and around 50–100 mSv for prolonged exposure (Yasser et al., 2020; Abbott et al., 2015; Tubiana et al., 2006). Below 50 mSv, there is no convincing epidemiological evidence of cancer risk.
The results of our study showed that high cumulative effective doses were due to the repetition of scans with multiple acquisitions, where doses were not sufficiently optimized.
It is thus necessary to raise awareness among physicians prescribing CT scans about patient radioprotection and the potential effects of ionizing radiation. Several studies indicate that the understanding of doses delivered during CT scans is often inadequate, and the risks associated with low doses of X-rays are largely underestimated (Benamar et al., 2023). A significant proportion of prescribers fail to consider the benefit-risk ratio when prescribing a CT scan (Amaoui et al., 2023, Najjar et al., 2022, Badiane et al., 2019, Ricketts et al., 2013). Broader dissemination of radioprotection training, particularly during the training of medical interns and residents, could be a solution to improve practitioners’ knowledge of patient radioprotection.
Furthermore, it would be relevant to revise CT scan protocols by reducing kV values and adjusting the scan length to the anatomy of the region to be examined, as well as monitoring and controlling the received doses to limit the cumulative impact of radiation. In general, it is essential to promote solutions based on a combination of technological, regulatory, and educational approaches.
The present study has certain limitations that may affect the validity of its conclusions, particularly the sample size and the fact that it focuses on a single center. However, the results of this study are noteworthy and draw attention to a subject that deserves further interest.
Dosimetric indicators found for the four types of examination.
5 Conclusion
The analysis of our results highlights the importance of strengthening the principle of justification for radiological examinations by ensuring that each examination is truly necessary and unavoidable for the patient.
Moreover, dose optimization remains a crucial issue in the patient radioprotection strategy to avoid or minimize the risks associated with the harmful effects of ionizing radiation. This strategy is based on several key measures, including:
Raising awareness among all stakeholders involved in patient care.
Digitizing medical records to make dosimetric information more accessible and facilitate exposure monitoring.
Providing ongoing training for radiology professionals, with periodic certification to ensure safe practices.
Implementing evidence-based practices and regularly updating diagnostic reference levels.
Promoting scientific research in fields related to the use of ionizing radiation in medicine, such as medical physics, radiobiology, signal processing, and artificial intelligence.
These measures aim to enhance patient safety and ensure a more responsible use of ionizing radiation in medical settings.
Acknowledgments
Authors are thankful to Miss. Bounouiss A, Mr. Kortobi I, and Mr. Lumbama E, for their commitment during data collection and Analysis.
Funding
This research did not receive any specific funding.
Conflicts of interest
The authors declare that they have no conflict of interest.
Data availability statement
Data associated with this article cannot be disclosed due to ethical reason.
Author contribution statement
Housni A: Study design, analysis, writing the original draft; Bounouiss A: Data collection and analysis; Kortobi I: Data collection and analysis; Lumbama E: Data collection and analysis; Amazian K: Statistical analysis, writing-reviewing; Essahlaoui A: Writing-reviewing; Labzour A: Writing-reviewing.
Ethics approval
Ethical approval was not required.
Informed consent
The article does not contain any studies involving human subjects.
References
- Abbott A. 2015. Researchers pin down risks of low-dose radiation. Nature 523: 17–18. [CrossRef] [PubMed] [Google Scholar]
- Abe K, Hosono M, Igarashi T, Iimori T, Ishiguro M, Ito T, Nagahata T, Tsushima H, Watanabe H. 2020. The 2020 national diagnostic reference levels for nuclear medicine in Japan. Ann Nucl Med 34: 799–806. [Google Scholar]
- Alashban Y, Shubayr N. 2023. Probability of induced cancers related to computed tomography examinations. Radiat Phys Chem 210: 111020. [CrossRef] [Google Scholar]
- Amaoui B, Safini F, Lahlou L, El Fahssi M, Abbaoui S, Semghouli S. 2023. Physicians’ knowledge about radiation protection of patients during prescription of CT scan procedures in Morocco. Radiat Med Prot 4 (1): 54–59. [CrossRef] [Google Scholar]
- Badiane SM, Sane PI, Ndiaye CN, Gueye K, Ndoye O, Amoussou-Guenou KM, Mbodji M. 2019. Evaluation of the knowledge of CT scan prescribers on patients’ radioprotection in Senegal. Open J Biophys 9: 204–217. [Google Scholar]
- Benamar M, Housni A, Sadiki S, Amazian K, Essahlaoui A, Labzour A. 2023. Patient dose assessment in computed tomography in a Moroccan imaging department. Radioprotection 58 (1): 49–53. [CrossRef] [EDP Sciences] [Google Scholar]
- Berrington de Gonzalez A, Mahesh M, Kim KP, et al. 2009. Projected cancer risks from computed tomography scans performed in the United States in 2007. Arch Intern Med 169: 2071–2077. [CrossRef] [PubMed] [Google Scholar]
- Bougana I, Benabdelouahab F, Loutfi A, Ouahrani AE. 2018. L’optimisation avec réduction de l’exposition du patient lors des procédures en scanographie TDM/TAP: cas des patients cancéreux au nord du Maroc. Radioprotection 53 (2): 115–122. [Google Scholar]
- Bourguignon M. 2021. Excessive patient doses through computed tomography imaging: new concerns. Radioprotection 56 (2): 89–90. [CrossRef] [EDP Sciences] [Google Scholar]
- Brenner DJ, Hall EJ. 2007. Computed tomography: an increasing source of radiation exposure. N Engl J Med 357: 2277–2284. [CrossRef] [PubMed] [Google Scholar]
- Dreuil S, Etard C. 2017 Exposure of the French population to ionizing radiations from medical diagnostic procedures in 2012. Radioprotection 52: 45–49. [CrossRef] [EDP Sciences] [Google Scholar]
- Dubousset J, Aurengo ADB., Cabanis EA, Chouard C, Morvan G, Brunelle F, Menkes CJ. 2016. De l’usage des Rayons X en radiologie (diagnostique et interventionnelle), à l’exclusion de la radiothérapie. Rapport et recommandations. Bulletin De L Academie Nationale De Medecine. [Google Scholar]
- Ekpo EU, Adejoh T, Akwo JD, Emeka OC, Modu AA, Abba M, Adesina KA, Omiyi DO, Chiegwu UH. 2018. Diagnostic reference levels for common computed tomography (CT) examinations : results from the first Nigerian nationwide dose survey. J Radiolog Protect 38: 525–535. [CrossRef] [PubMed] [Google Scholar]
- El Mansouri M, Talbi M, Choukri A, Nhila O, Aabid M. 2022. Establishing local diagnostic reference levels for adult computed tomography in Morocco. Radioprotection 57 (1): 61–66. [CrossRef] [EDP Sciences] [Google Scholar]
- Frija G, Damilakis J, Paulo G, Loose R, Eliseo V, European Society of Radiology (ESR). 2021. Cumulative effective dose from recurrent CT examinations in Europe: proposal for clinical guidance based on an ESR EuroSafe Imaging survey. Eur Radiol 31 (8): 5514–5523. [Google Scholar]
- ICRP. 2007. The 2007 recommendations of the international commission on radiological protection. ICRP Publication 103. Annals ICRP 37: 1–332. [Google Scholar]
- ICRP. 1991. The 1990 recommendations of the international commission on radiological protection. ICRP Publication 103. Annals ICRP 21: 1–3. [Google Scholar]
- IRSN. 2023. Analysis of data for updating diagnostic reference levels in radiology and nuclear medicine: 2012 report. [Google Scholar]
- IRSN. 2020a. Exposition de la population aux rayonnements ionisants due aux actes d’imagerie médicale diagnostique réalisés en France en 2017. https://www.irsn.fr/FR/expertise/rapports_expertise/Documents/radioprotection/IRSN_Rapport_Expri_2019.pdf. [Google Scholar]
- Karim MKA, Hashim S, Bradley DA, Bakar KA, Haron MR, Kayun Z. 2016. Radiation doses from computed tomography practice in Johor Bahru, Malaysia. Radiat Phys Chem 121: 69–79. [Google Scholar]
- Laurier D, Richardson DB, Cardis E, Daniels RD, Gillies M, O’Hagan J, Hamra GB, Haylock R, Leuraud K, Moissonnier M, Schubauer-Berigan MK, Thierry-Chef I, Kesminiene A. 2017. The international nuclear workers study (Inworks): a collaborative epidemiological study to improve knowledge about health effects of protracted low-dose exposure. Radiat Prot Dosimetry 173 (1-3): 21–25. [Google Scholar]
- Lee KL, Beveridge T, Sanagou M, Thomas P. 2020. Updated Australian diagnostic reference levels for adult CT. Med Imaging Radiat Sci 67 (1): 5–15. [CrossRef] [PubMed] [Google Scholar]
- Little MP. 2009. Cancer and non-cancer effects in Japanese atomic bomb survivors. Radiol Prot 29(2A): A43–A59. [Google Scholar]
- Najjar RH, Alsulaiman AM, Alraddadi JS, Alrohaimi NH, Algarni BA, Al-Arafa AM, Alsubait RA. 2022. Assessment of physicians’ knowledge and awareness about the hazards of radiological examinations on the health of their patients at a Tertiary Care Hospital, Riyadh, Saudi Arabia. Cureus 14 (7): e27479. [Google Scholar]
- Oikarinen H, Meriläinen S, Pääkkö E, Karttunen A, Nieminen MT, Tervonen O. 2009. Unjustified CT examinations in young patients. Eur Radiol 19 (5): 1161–1165. [Google Scholar]
- Rehani MM, Heil J, Baliyan V. 2021. Multicentric study of patients receiving 50 or 100 mSv in a single day through CT imaging-frequency determination and imaging protocols involved. Eur Radiol 31 (9): 6612–6620. [Google Scholar]
- Ricketts ML, Baerlocher MO, Asch MR, Myers A. 2013. Perception of radiation exposure and risk among patients, medical students, and referring physicians at a tertiary care community hospital. Can Assoc Radiol J 64 (3): 208–212. [Google Scholar]
- Schegerer A, Loose R, Heuser LJ, Brix G. 2019. Diagnostic reference levels for diagnostic and interventional X-ray procedures in Germany: update and handling. Rofo 191 (8): 739–751. [CrossRef] [PubMed] [Google Scholar]
- Shubayr N, Alashban Y. 2023. Estimation of radiation doses and lifetime attributable risk of radiation-induced cancer in the uterus and prostate from abdomen pelvis CT examinations. Front Public Health 10: 1094328. [Google Scholar]
- Smith-Bindman R, Kwan ML, Marlow EC, Theis MK, Bolch W, Cheng SY, Bowles EJA, Duncan JR, Greenlee RT, Kushi LH, Pole JD, Rahm AK, Stout NK, Weinmann S, Miglioretti DL. 2019. Tends in use of medical imaging in US health care systems and in Ontario, Canada, 2000–2016. JAMA 322 (9): 843–856. [CrossRef] [PubMed] [Google Scholar]
- Tubiana M, Aurengo A, Averbeck D, Masse R. 2006, Recent reports on the effect of low doses of ionizing radiation and its dose-effect relationship. Radiat Environ Biophys 44: 245–251. [CrossRef] [PubMed] [Google Scholar]
- Venneri L, Rossi F, Botto N, Andreassi MG, Salcone N, Emad A, Lazzeri M, Gori C, Vano E, Picano E. 2009. Cancer risk from professional exposure in staff working in cardiac catheterization laboratory: insights from the national research council’s biological effects of ionizing radiation vii report. Am Heart J 157 (1): 118–124. [CrossRef] [PubMed] [Google Scholar]
- Yasser A, Francis C, Liu N-A., Guangming Z. 2020. Cancer risk of low dose ionizing radiation. Front Phys Sec Med Phys Imag 8–2020. [Google Scholar]
Cite this article as: Housni A, Bounouiss A, Kortobi I, Lumbama E, Amazian K, Essahlaoui A, Labzour A. 2026. Assessment of the cumulative dose in computed tomography (CT) in Moroccan hospitalized patients. Radioprotection 61(1): 48–54. https://doi.org/10.1051/radiopro/2025025
All Tables
Distribution of the values of the volumetric CT dose index (CTDIvol) (mGy) per acquisition for each CT scan type.
Distribution of the values of the dose length product (DLP) (mGy.cm) per acquisition for each CT scan type.
Distribution of the values of the Volumetric CT dose index (CTDI vol) (mGy) per patient over one year for each CT scan type.
Distribution of the values of the dose length product (DLP) (mGy.cm) per patient over one year for each CT scan type.
All Figures
|
Fig. 1 Distribution of the cumulative annual effective dose per patient. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.