")
")
| Issue |
Radioprotection
Volume 61, Number 2, Avril-Juin 2026
|
|
|---|---|---|
| Page(s) | 171 - 177 | |
| DOI | https://doi.org/10.1051/radiopro/2025031 | |
| Published online | 15 June 2026 | |
Article
Survey following uranium contamination
1
CEA, Service de Prévention et Santé au Travail, 13115 Saint-Paul-Lez-Durance Cedex, France
2
CEA, Département des Services de Santé et Sécurité, 13115 Saint-Paul-Lez-Durance Cedex, France
3
CEA, Service de Protection contre les Rayonnements, 13115 Saint-Paul-Lez-Durance Cedex, France
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
13
June
2025
Accepted:
7
September
2025
Abstract
Any discrepancy between the initially hypothesis of an occupational exposure and the additional information collected from the facility and the radiation protection team should lead the exploration of other issues. In this specific case, the hypothesis of occupational intake in Uranium was selected based on the biokinetic models but not validated by the examination of the workplace. Additional information on the worker’s dietary habits helped us understand the origin of the radiotoxicological monitoring results for Uranium exceeding the commonly accepted thresholds for the non-occupationally exposed general population.
Key words: Uranium / dose assessment / dietary intake / phosphoric acid / chemical form
© N. Blanchin et al., Published by EDP Sciences 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
1 Introduction
Uranium is a ubiquitous atom in the Earth’s crust. It is thus naturally found in food and drinking water (Ministère de la Santé − France, 2011). It is absorbed into the blood, from which it is filtered by the kidneys and eliminated in the urine. This mechanism leads to detectable activities in the excreta of the general population not professionally exposed. Uranium in the blood also deposits in the bone (cortical and trabecular zones) and in the liver. Its concentration due to diet varies greatly depending on the place of residence and dietary habits (ICRP, 1995). The solubility of the compound is the predominant factor to know the target organ and predict its toxicity. Unlike soluble uranium compounds from ore processing, whose toxicity is chemical in nature and notably affects the kidney, oxide forms are less soluble and the toxicity is rather radiological, historically responsible for bronchopulmonary cancers in case of inhalation, in combination with radon (Métivier, 2001).
Uranium is the main compound of nuclear fuels based on fission. Monitoring of workers professionally exposed to uranium relies, in addition to surface and atmospheric monitoring at the workplace, on individual monitoring from radiotoxicological analyses of excreta (urine and feces). Thus, the result of a radiotoxicological analysis of uranium in a person professionally exposed to uranium depends on the dietary intake to which may be added an incorporation of professional origin (Blanchin et al., 2013; Davesne et al., 2014).
This case illustrates the difficulty, in certain situations, of determining the professional or non-professional origin of a uranium activity detected in a worker’s excreta. When these activities exceed the thresholds commonly accepted in the general population, it is necessary to be systematic in the investigation allowing to determine the conditions and parameters of incorporation.
2 Discovery of abnormal uranium contamination in a decontamination worker
Mr CC, a worker employed by a company specializing in cleanup operations related to nuclear decommissioning has been working on various installations at Cadarache site since 2009. He is subject to systematic alpha radiotoxicological monitoring due to the risk of exposure to plutonium, americium, and uranium at the different worksites where he operates. This worker exhibited, in April 2015 and February 2016, urinary excretion of uranium slightly above the environmental background level. Subsequent tests returned results below the detection limit (see Tab. 2)
In July 2016, a radiotoxicological analysis of 24-hour urine showed a value of 11 mBq, exceeding levels considered normal in the general population and attributed to dietary intake. The reference document "Surveillance médico-professionnelle de l’exposition interne aux radionucléides en INB” (SFMT, 2011) establishes a benchmark value of 1.25 mBq/L, which corresponds to an activity between 1 and 3 mBq over 24 hours depending on daily diuresis (Recommendation 54). This value is also much higher than the upper values (0.034 μg/l, equivalent to 0.9 mBq/l) found in the French population in the ESTEBAN study over the period 2014-2016 (Esteban study, France 2024)
The isotopic ratio U234/U238 in this analysis was 1.2, consistent with natural isotopy. The same Recommendation 54 (SFMT, 2011) defines natural isotopy as an isotopic ratio U234/U238 below 2.
Simultaneously, a radiotoxicological analysis of 24-hour feces samples was conducted, yielding a result of 19.4 mBq. Current best practice guidelines (SFMT, 2011) use 45 mBq/24 h as the reference value for activity linked to dietary intake. This result therefore falls within the normal range observed in the general population (see Tab. 1).
Furthermore, it should be noted that the analysis results for plutonium and americium in the same samples are below the laboratory’s usual detection limits (0.2 mBq for 24-hour urine and 1 mBq for 24-hour feces samples).
Uranium bioassay results of the involved worker.
Control bioassay results of the involved worker.
3 Further information from the employee
Following these initial results, the employee was examined by the physician for information gathering and an interview:
Regarding any possible contamination event that may have occurred since the previous “normal” analysis.
Regarding his dietary habits, in particular the type of mineral water consumed or the use of a well (Mineral water and radioactivity Technical report, 2000) as well as the intake of certain clay-based medications, which are widely used by the general population in cases of diarrhea. The employee was also questioned about the consumption of mushrooms or wild plants known to concentrate certain elements, including uranium.
Regarding the first, professional aspect, no specific event could be identified by the employee. However, this issue will require further investigation by the radioprotection teams (see paragraph 5).
Regarding the consumption of mineral water, the employee states that he only drinks tap water. It should be noted that a survey conducted on a control population of workers at Cadarache from 2001 to 2011 (Blanchin et al., 2013; Davesne et al., 2014) showed a very high variability in urinary and fecal excretion, both between individuals (inter-individual) and for the same individual from one analysis to another (intra-individual). Out of approximately 600 urine analyses, nearly 90% of the results were below the detection limits at the time (between 1 and 3 mBq), and it was found that the Cadarache population did not differ from the French reference data. This is not surprising given the predominantly limestone nature of the soil in Provence, which results in low uranium concentrations in the soil and consequently in tap water.
Finally, the employee informed us that he is neither a hunter nor a gatherer of mushrooms or wild herbs, and furthermore, he is not undergoing any treatment, particularly for digestive issues.
Given these initial findings, the physician decided to schedule more frequent radiotoxicological tests in order to support a possible occupational origin.
Furthermore, the radiotoxicological analysis results of all employees working on the same sites as Mr CC were carefully reviewed. No similar findings were observed.
4 Additional investigations
The results of the radiotoxicological samples are presented in Table 2 below. LOD means “limit of detection” and is the lowest measurable activity.
The date of 11/04/2016 corresponds to the last test result below the laboratory’s detection limits and therefore represents the potential start date of exposure, which is the most unfavorable scenario from a dosimetric perspective.
It is observed that all 24-hour urine radiotoxicological analysis results from July 2016 onwards are significantly higher than the values seen in the general population and those considered to be related to dietary intake.
Conversely, over the same period, all 24-hour feces radiotoxicological analysis results fall within the normal range for the general population.
5 Interpretation of results and provisional dosimetric estimate
Given the absence of any indications of possible contamination, two scenarios were considered: an acute occupational inhalation or a chronic dietary ingestion.
First scenario: This is the default scenario, involving acute inhalation exposure that occurred on 12/04/2016 (the date of the previous analysis < LOD) to a uranium oxide compound, type S, according to the "inhalation" model of ICRP 78 (Marsh et al., 2007), which was the reference biokinetic model at the time (see Fig. 1)
The curves are generated by the IMBA software (Birchall et al., 2006) :
The blue points correspond to the measured values in urine on the upper graph and in feces on the lower graph. The measured values are associated with an uncertainty value defined by the scattering factor (SF) (Marsh et al., 2007)). IDEAS Guidelines (Castellani et al., 2013, 2016) recommends using an SF value of 1.1 for 24-hour urine samples and 3 for 24-hour feces samples. The SF is represented by the uncertainty bars around the data points.
The green curves correspond to the biokinetic model from ICRP Publication 78 (ICRP, 1997) used as the hypothesis (acute inhalation).
In this first scenario, there is good correlation, confirmed by the chi-squared test, between the measurement results and the theoretical curves of the ICRP model used as the hypothesis (acute inhalation).
In this scenario, the intake is estimated at approximately 3000 Bq, corresponding to a committed effective dose of 18.5 mSv. It should be noted that this hypothesis − which assumes the potential incorporation date as the day after the previous urine analysis < LOD − represents a worst-case assumption. Additionally, the dietary background contribution was not subtracted from the feces results, as advised in Good Practice Recommendation 54 (SFMT, 2011).
Nevertheless, this initial estimate provides an order of magnitude for the committed effective dose, which approaches the annual regulatory limit set in France (20 mSv for category A employees) aligned with ICRP recommendations for radiation workers.
Consequently, meticulous investigations will be conducted by the radioprotection service to determine the possible origin of the contamination. Specifically, all of Mr CC’s activities in radiological areas since 12/04/2016 have been tracked, along with any potential contamination incidents that occurred during this period. All nasal mucus samples, atmospheric contamination measurements, and surface contamination measurements during this timeframe returned "negative" results.
Finally, all facilities where Mr. CC worked had mixed radioactive spectra, primarily containing plutonium and americium, combined with uranium. Mr. CC never worked in facilities where the source term consisted exclusively of uranium. None of the radiotoxicological analyses performed detected the presence of transuranic elements.
Although the interpretation of results relative to the ICRP theoretical models (8) supports an occupational inhalation origin, no evidence from the radioprotection team’s worksites investigation corroborated this hypothesis. Furthermore, the two significant positive urine test results from April 2015 and February 2016, followed by negative follow-up tests, cannot be explained by pre-April 2015 inhalation contamination.
Second scenario: chronic dietary origin, involving an unspecified compound with f1 = 0.02, according to the “ingestion” model from ICRP Publication 78 (ICRP, 1997), the reference biokinetic model at the time (see Fig. 2)
It is observed that while the theoretical curve fits well with the urine measurement results, there is a discrepancy with the feces measurement results. The statistical test (chi-squared test) confirms the poor fit of the selected model with the data points. In practice, given the urinary values, the feces results should be ten times higher than those measured.
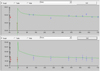 |
Fig. 1 Graphical representation of urinary measurements compared to predicted values with the ICRP 78 biokinetic model for inhalation (IMBA). |
 |
Fig. 2 Graphical representation of urinary measurements compared to predicted values with the ICRP 78 biokinetic model for ingestion (IMBA). |
6 Important additional information leading to new interpretation hypotheses
In early 2018, a radiation protection officer from Mr CC’s company, involved in the occupational investigation, provided new information about Mr. CC: he consumed several liters of cola daily (averaging 2L per day). Mr. CC confirmed this detail, which had not been disclosed during his initial interviews that focused primarily on his mineral water consumption.
We first focused on the chemical composition of this type of beverage. The label on a bottle of the implicated soda lists the following components:
Carbonated water.
Coloring agent : E150d (caramel color).
Acidifiers : phosphoric acid, sodium citrate.
Sugar or sweeteners : aspartame, acesulfame-K.
Natural flavors, including caffeine.
Additionally, a quick inquiry with the manufacturer revealed that the water used in production across different sites comes from the local distribution network. The uranium content is therefore presumed identical to the region’s tap water. Nevertheless, a radiotoxicological analysis of a sample of the cola consumed by Mr CC was conducted by Cadarache medical analysis laboratory. The measured activity in this sample was 25 mBq/L, a value close to that of Volvic water, which is recognized as one of the least mineralized waters in France. By comparison, the most "radioactive" waters in France exhibit levels over 100 times higher than this cola sample (Mineral water and radioactivity Technical report, 2000). The hypothesis of elevated uranium content in the cola was thus ruled out.
However, chemistry colleagues at Cadarache urged us to investigate the cola hypothesis due to its chemical composition, particularly the presence of phosphoric acid, which is known for its affinity with uranium (see discussion below).
Mr CC was therefore asked to repeat radiotoxicological analyses after abstaining from cola for several days. The April 2018 test results showed a return to usual values for the general population (<1.25 mBq/L). See Table 3.
Then Mr CC’s urinary radiotoxicological analyses have always remained within the normal values for the general population (< 3 mBq / 24 h).
The radiotoxicological analyses of the feces samples have likewise remained unchanged, within the usual values observed in the general population and consistent with dietary intake.
The hypothesis of increased gastrointestinal absorption of uranium due to the chemical composition of cola was therefore proposed. By increasing the digestive absorption factor f1 tenfold (from 0.02 to 0.2) in the ICRP Publication 78 biokinetic model, an excellent correlation (fit) was achieved between the theoretical curves and the urine and feces results from July 2016 to March 2018 (see Fig. 3)
In this scenario, the estimated average intake is 40 mBq/day, which aligns with dietary intake primarily linked to Mr CC’s consumption of cola (approximately 25 mBq/L).
The committed effective dose is estimated at 12.5 μSv over the studied period (approximately 2 yr).
Regarding the chemical toxicity of uranium on the kidneys, France’s INRS indicates (INRS, 2024) a urinary excretion value of 250 μg/L (equivalent to 6.25 Bq/L) beyond which renal impairment can occur. The urinary activity levels measured in Mr. CC were well below this reference value.
Similarly, the World Health Organization (World Health Organization, 2022) recommends a guideline value of 30 µg/L for uranium concentration in drinking water, equivalent to 750 mBq/L. This value corresponds to an annual committed effective dose of 0.10 mSv, assuming a daily consumption of 2 liters of water.
The Table 4 summarizes recommended values from WHO, in the United States of America and in Canada.
The values found in the implicated cola-type beverage, based on analyses performed by the Cadarache laboratory, are also well below these levels. It should be noted, however, that these values can be exceeded in certain mineral waters (Mineral water and radioactivity Technical report, 2000), whose consumption should therefore be limited.
Last bioassay results in the involved worker.
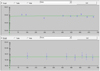 |
Fig. 3 Graphical representation of urinary measurements compared to predicted values with the ICRP 78 biokinetic model for ingestion with a revised f1 factor. |
Summary of standards and recommendations for uranium intake in drinking water.
7 Discussion − Hypotheses on explanatory mechanism
The metabolism of ingested uranium is not as well understood as that of radium. Wrenn and colleagues (Wrenn et al., 1985) estimated that approximately 1.1% of ingested uranium is absorbed through the gastrointestinal tract.
The observed increase in digestive absorption of uranium may be linked to the chemical composition of the beverage, particularly the presence of phosphoric acid. Phosphoric acid forms from the reaction of phosphorus with oxygen and water and subsequently recombines into various inorganic or organic phosphates (Wagner et al., 2023). Phosphate metabolism is associated with several key biological functions, including phospholipid metabolism, bone mineralization, adenosine triphosphate (ATP, the cellular energy carrier), and others. In their work, Leggett and Harrison (Leggett et al., 2095) emphasize, based on laboratory data from animal studies, that the absorbed fraction of uranium strongly depends on its ingested chemical form.
Numerous studies demonstrate uranium’s affinity with phosphates, whether in solid form (e.g., uranium’s presence in phosphate fertilizers or natural minerals like apatite and monazite) or in solution. In such environments, the formation of uranium-phosphate complexes such as UO2H2PO4+, UO2(H2PO4)2 et UO2(H2PO4)2(H3PO4) has been demonstrated in phosphoric acid (Dartiguelongue, 2014).
Calculations of uranium speciation in human biological fluids conducted by Sutton and Burastero (Sutton et al., 2004) show the different chemical forms of uranium in solution, depending on the fluids’ chemical composition :
Carbonate complexes in carbonate-rich fluids
UO2(CO3)34- in plasma at pH 7.4
UO2(CO3)34- and UO2(CO3)22- in the pancreas at pH 8.3
Hydroxylated forms UO2(OH)2 in saliva at pH 6–7
Phosphate forms in fluids richer in phosphates, such as urine
UO2(HPO4)22- at pH 4,2 et 8.
In gastric juice, which is less rich in phosphates, the speciation of uranium varies significantly depending on pH :
UO22- at pH 1 toUO2(HPO4)22- at pH 3,5.
Thus, it can be suggested that the high concentration of phosphoric acid in the carbonated beverage promotes the formation of UO₂(HPO₄)₂2⁻ in gastric juice, displacing the UO₂2⁻ form. As shown in various studies (Sandino et al., 2005; Sutton et al., 2004), this chemical form (UO₂(HPO₄)₂2⁻) has a high solubility.
Moreover, data from animal studies provide information on the relative uptake of uranium ingested in different chemical forms, showing that absorption is strongly dependent on the solubility of the compound (ICRP, 2017)
So, we can assume that uranium in this chemical form (UO₂(HPO₄)₂2⁻) has a higher solubility, thereby enhancing gastrointestinal absorption compared to classic hydroxylated or carbonated chemical forms.
8 Conclusion
This clinical case highlights the critical importance, in dosimetric interpretation, of always cross-referencing hypotheses with data from employee interviews and supplementary information provided by the facility and radioprotection teams.
Any inconsistency between exposure data and the proposed biokinetic model − even if it shows excellent correlation between theoretical curves and measured results − should prompt a re-evaluation of the model and exploration of alternative hypotheses.
This necessitates multidisciplinary collaboration, leveraging expertise across fields such as biology, chemistry, mathematics, and radioprotection.
In this instance, such collaboration advanced understanding of how certain foods (e.g., cola) influence gastrointestinal uranium absorption. Subsequent cases have confirmed cola’s impact on urinary uranium excretion, making its consumption a routine inquiry when analyses exceed general population background levels.
As the medical adage goes: “You only find what you look for, and you only look for what you already know.”
Acknowledgements
In memory of our colleague and friend Philippe Bérard (1952–2020), one of the world's leading experts on uranium.
Funding
This research did not receive any specific funding.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Data availability statement
Research data are included within the article.
Ethics approval
Ethical approval was not required.
Informed consent
Written informed consent has been obtained from the patient.
References
- Base de données Biotox − Publications et outils − INRS. Disponible sur: https://www.inrs.fr/publications/bdd/biotox.html [Google Scholar]
- Birchall A, Puncher M, Marsh JW, Davis K, Bailey MR, Jarvis NS, et al. 2006. IMBA professional plus: a flexible approach to internal dosimetry. Radiat Prot Dosim 125(1‑4): 194–197. [Google Scholar]
- Blanchin N, Davesne E, Chojnacki E, Touri L, Ruffin M, Blanchardon E. 2013. Interprétation des résultats de surveillance individuelle des expositions professionnelles au dioxyde d’uranium «Proposition de dosimétrie collective». Radioprotection 48 (3): 411–430. [Google Scholar]
- Castellani CM, Marsh JW, Hurtgen C, Blanchardon E, Berard P, Giussani A, et al. 2013. IDEAS Guidelines (Version 2) for the Estimation of Committed Doses from' Incorporation Monitoring Data [Internet]. European Radiation Dosimetry Group e.V. EURADOS-Report- 2013-01. p. 2.4 MB. Disponible sur: https://eurados.sckcen.be/sites/eurados/files/uploads/Publications/24. [Google Scholar]
- Castellani CM, Marsh JW, Hurtgen C, Blanchardon E, Bérard P, Giussani A, et al. 2016. EURADOS-IDEAS Guidelines (Version 2) for the estimation of committed doses from incorporation monitoring data. Radiat Prot Dosim 170(1‑4): 17–20. [Google Scholar]
- Dartiguelongue A. 2014. Etude de la spéciation de l’uranium(VI) dans les solutions d’acide phosphorique et de sa récupération par extraction liquide-liquide [Internet] [phdthesis]. ENSTA ParisTech; [cité 11 oct 2024]. Disponible sur: https://pastel.hal.science/tel-01244583. [Google Scholar]
- Davesne E, Blanchin N, Chojnacki E, Touri L, Ruffin M, Blanchardon E, et al. 2014. Collective dosimetry to distinguish occupational exposure to natural uranium from alimentary uranium background in bioassay measurements. Int J Radiat Biol 90 (11): 1048–1054. [Google Scholar]
- Esteban study, France 2024. [Google Scholar]
- Groupe de travail Methode Dosimétrique de Référence (collectif). 2011. Surveillance médico-professionnelle de l’exposition interne aux radionucléides en installations nucléaires de base [Internet]. SFMT. Disponible sur: https://www.societefrancaisedesanteautravail.fr/page-33/recommandations-de-la-sfst. [Google Scholar]
- Individual Monitoring for Internal Exposure of Workers. 1997. ICRP Publ 78 27(3‑4): 1–161. [Google Scholar]
- INRS; 2024 - Base de données Biotox Publications et outils .sur: https://www.inrs.fr/publications/bdd/biotox.html [Google Scholar]
- Leggett R, Harrison J. 1995. Fractional absorption of ingested uranium in humans. Health Phys [Internet]. [cité 11 oct 2024];68(4). Disponible sur: https://pubmed.ncbi.nlm.nih.gov/7883560/ [Google Scholar]
- Marsh J, Blanchardon E, Castellani C, Desai A, Dorrian M, Hurtgen C, et al. 2007. Evaluation of scattering factor values for internal dose assessment following the IDEAS guidelines: preliminary results. Radiat Prot Dosim. [cité 11 oct 2024];127(1‑4). Disponible sur: https://pubmed.ncbi.nlm.nih.gov/18045799/. [Google Scholar]
- Métivier H (coordination éditoriale). 2001. L’uranium − De l’environnement à l’homme. 1ère édition. EDP Sciences; [cité 11 oct 2024]. (Institut de Radioprotection et de SÛreté Nucléaire). Disponible sur: https://laboutique.edpsciences.fr/produit/349/9782868835307/l-uranium. [Google Scholar]
- Ministre de la Sant Français - rapport 2011 [Google Scholar]
- Occupational Intakes of Radionuclides (OIR). 2017. Part 3 − ICRP Publ 13. 15.2.2 Ingestion. [Google Scholar]
- Rapport du Ministère de la Santé Français. 2011. ASN − IRSN − Qualité radiologique de l’eau du robinet en France. [Google Scholar]
- Results from the Esteban study. 2024. Exposure of the general French population to metals and metalloids in 2014–2016. Environ Res 252(Part 2). [Google Scholar]
- Sandino et al., The solubility of Uranium phosphate and the formation of Uranium phosphate complexes - Environmental Science, Chemistry – 2005. [Google Scholar]
- Sutton M, Burastero SR. 2004. Uranium(VI) solubility and speciation in simulated elemental human biological fluids. Chem Res Toxicol 17 (11): 1468–1480. [Google Scholar]
- Wagner CA. 2023. The basics of phosphate metabolism. Nephrol Dial Transplant. gfad188. [Google Scholar]
- World Health Organization, éditeur. 2022. Guidelines for drinking-water quality. Fourth edition, World Health Organization. 614p. [Google Scholar]
- Wrenn ME, Durbin PW, Howard B, Lipsztein J, Rundo J, Still ET, et al. 1985. Metabolism of ingested U and Ra. Health Phys 48 (5): 601–633. [Google Scholar]
Cite this article as: Blanchin N, Grare R, Guy C, Halladjian L. 2026. Survey following uranium contamination. Radioprotection 61(2): 171–177. https://doi.org/10.1051/radiopro/2025031
All Tables
All Figures
|
Fig. 1 Graphical representation of urinary measurements compared to predicted values with the ICRP 78 biokinetic model for inhalation (IMBA). |
| In the text | |
|
Fig. 2 Graphical representation of urinary measurements compared to predicted values with the ICRP 78 biokinetic model for ingestion (IMBA). |
| In the text | |
|
Fig. 3 Graphical representation of urinary measurements compared to predicted values with the ICRP 78 biokinetic model for ingestion with a revised f1 factor. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.