")
")
| Issue |
Radioprotection
Volume 61, Number 1, Janvier-Mars 2026
|
|
|---|---|---|
| Page(s) | 62 - 67 | |
| DOI | https://doi.org/10.1051/radiopro/2025023 | |
| Published online | 20 March 2026 | |
Article
Assessment of radiation risk associated with whole-body computed tomography at the emergency department
Diagnostic Radiography Technology, College of Nursing and Health Sciences, Jazan University, Jazan, Saudi Arabia
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
25
December
2024
Accepted:
7
August
2025
Abstract
Whole-body computed tomography (WBCT) is a standard diagnostic imaging tool used for the urgent evaluation of patients with serious traumatic injuries. However, the use of WBCT for screening patients suspected of having multiple blunt traumas remains controversial due to the excessive radiation exposure involved. This study aimed to estimate effective and organ equivalent doses and evaluate the lifetime attributable risk (LAR) of cancer incidence and mortality resulting from WBCT examinations for trauma patients. Data, including patients’ demographic and exposure parameters, were collected retrospectively from the picture archiving and communication system for 175 traumatic patients. National Cancer Institute CT (NCICT) software was used to calculate the organ doses and effective doses. The age- and sex-specific LAR incidence and mortality for organ doses were calculated via risk models proposed by the BEIR VII report. The overall mean effective radiation dose for trauma patients who underwent WBCT was 20.81 ± 10.78 mSv. Compared with males, females had a greater mean dose (21.95 ± 11.72 mSv) (18.93 ± 8.73 mSv). The organ doses ranged from 1.76–37.69 mGy for females and from 1.26–32.79 mGy for males. Females face higher lifetime cancer risk (incidence 0.70%, mortality 0.40%) than males do (incidence 0.60%, mortality 0.32%). The overall lifetime cancer risk was 0.65% for incidence and 0.36% for mortality. WBCT scanning involves significant radiation exposure and carries a risk of developing cancer. Therefore, the use of WBCT should be clinically justified, and measures should be taken to reduce the radiation dose.
Key words: Computed tomography / emergency department / trauma / whole-body
© N. Shubayr, Published by EDP Sciences 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
1 Introduction
Whole-body computed tomography (WBCT) has become an essential diagnostic procedure in the initial evaluation and management of patients with multiple traumatic injuries. The use of WBCT allows for rapid and comprehensive assessment of injuries, enabling timely diagnosis and treatment decisions that can improve patient outcomes (Mulas et al., 2022). According to a recent retrospective multicenter study, using WBCT as the primary imaging modality for patients with multiple types of trauma significantly improves their chances of survival compared with a selective imaging approach that uses radiography, sonography, and CT of specific body regions (Huber-Wagner et al., 2009; Jiang et al., 2014). As a result, research has recommended using WBCT as the primary diagnostic tool for trauma patients, even in cases where the patient’s hemodynamic stability is borderline (Huber-Wagner et al., 2018). However, the increased utilization of WBCT in trauma settings has raised concerns about the potential risks associated with radiation exposure, particularly in younger patients, who are more susceptible to the long-term effects of ionizing radiation (Wen et al., 2013; Weber et al., 2023).
The radiation dose from WBCT scans can vary significantly depending on the scanning protocol, patient characteristics, and CT scanner technology used (Gordic et al., 2015; Zensen et al., 2022). Trauma patients often require multiple CT scans during their hospital stay, which can result in cumulative radiation doses that exceed those of the general population (Moorin et al., 2014). Therefore, it is crucial to assess and optimize radiation doses in WBCT protocols for multiple injured patients to minimize potential risks while maintaining diagnostic accuracy.
Several studies have investigated the radiation dose associated with WBCT in trauma patients. Sierink et al. reported that the mean effective dose for a single WBCT scan was 20.6 mSv, which is equivalent to approximately 1,000 chest X-rays (Sierink et al., 2016). Brenner and Elliston estimated that a single WBCT scan with an effective dose of 12 mSv in a 45-year-old patient could increase the lifetime attributable risk (LAR) of cancer by 0.08% (Brenner et al., 2004). These findings highlight the importance of implementing dose reduction strategies and optimizing WBCT protocols to minimize radiation exposure while maintaining diagnostic quality.
The estimation of the associated radiation-induced risks helps to provide some direction in terms of CT dose optimization. The radiation dose, especially to the abdomen and pelvis, involves relatively radiosensitive organs and tissues such as the testes, ovaries, small intestines, rectum, bladder, and uterus. Additionally, organs and tissues with low to intermediate radiosensitivity, including the pancreas, kidneys, and adrenal glands, are exposed to radiation. Accordingly, the abdominal and pelvis organs account for 50% of the tissue radiosensitivity (ICRP, 2007). It is crucial to understand how much radiation is supplied to patients during CT procedures to balance the probability of harm and the potential benefits properly. This is especially important because the CT usage has become less restrictive, resulting in increased utilization among healthy individuals, where the potential risks of CT-related carcinogenesis could surpass its diagnostic benefits (Kim et al., 2010). Research investigating radiation exposure from WBCT and associated cancer risk among trauma patients in Saudi Arabia is limited. Therefore, this study aimed to estimate effective and organ equivalent doses and evaluate the LAR of cancer incidence and mortality resulting from WBCT examinations for trauma patients.
2 Methods and materials
2.1 Study design and setting
This study was a retrospective analysis conducted at a general hospital in Saudi Arabia. The aim of this study was to investigate the radiation risk associated with WBCT scans in trauma patients. The hospital’s radiology department used a General Electric (GE) Lightspeed 16-slice CT scanner for imaging.
2.2 Study population and data collection
The study included adult patients who were admitted to the emergency department and underwent WBCT scans (head, neck, chest, abdomen, and pelvis) for trauma-related indications. Patient demographic information, such as age, sex and body mass index, was collected (Tab. 1). A picture archiving and communication system (PACS) was used to gather data for patients with indications suggestive of trauma, including motor vehicle accidents, falls, and assaults. The scans were completed in two separate protocols: (a) head and (b) neck, chest, abdomen, and pelvis. The collected data included WBCT exposure parameters as reported in the CT radiation dose report. Head and neck were scanned first, followed immediately by a contiguous neck-to-pelvis helical acquisition; CTDIvol and DLP for the two series were summed before entering NCICT.
Demographic characteristics of study participants.
2.3 Radiation dose assessment
National Cancer Institute CT (NCICT) dosimetry software was used to calculate organ doses and effective doses in millisieverts (mSv) for the total number of scans (Lee et al., 2015). The software requires various patient and exposure parameters for dose calculation, such as patient age, sex, height, weight, scan range, scanner manufacturer and model, filter (head/body), tube potential (kVp), current × time (mAs), pitch, and CTDIvol.
2.4 Radiation risk estimation
The risk models proposed by the BEIR VII (2006) report describe a technique to approximate the LAR of cancer on the basis of the amount of a single radiation dose and a patient’s age and sex (NRC, 2006). The LAR is defined as an additional cancer risk above and beyond the baseline cancer risk. The calculated organ doses were used to estimate the age- and sex-specific LAR cancer incidence and mortality rates via BEIR VII risk estimates.
2.5 Statistical analysis
The statistical analysis was performed via the Statistical Package for the Social Sciences (SPSS version 26, IBM Inc., Chicago, IL). Continuous variables are reported as the means ± standard deviations, whereas categorical variables are presented as frequencies and percentages. Independent samples t tests were used to compare variables, with p < 0.05 considered statistically significant.
3 Results
The total study population included 175 participants, including 109 males (62.3%) and 66 females (37.7%). As shown in Table 2, the CTDIvol had a mean value of 16.03 ± 8.13 mGy, with a 50th percentile of 15.9 mGy and an interquartile range (25th–75th percentile) of 9.3–21.13 mGy. The mean DLP was 1063.21 ± 523.5 mGy · cm, with a 50th percentile of 1043 mGy · cm and an interquartile range of 633–1456.5 mGy · cm. The overall mean effective dose for all trauma patients who underwent a WB CT scan was 20.81 ± 10.78 mSv, with a range of 3.10–64.7 mSv.
The mean effective dose from trauma-related WBCT scans for female patients (21.95 ± 11.72 mSv) was greater than that for male patients (18.93 ± 8.73 mSv), with a p value of 0.019, indicating a statistically significant difference. Figure 1 shows how effective radiation doses are distributed between male and female patients. The distribution for female patients exhibited a pronounced right skew, suggesting a scarcity of high doses despite a broader range. In contrast, male patients’ radiation doses are more centrally distributed, with a less pronounced right skew, indicating less variability in their exposure levels.
Figure 2 presents the radiation doses received by various organs in female and male patients undergoing WBCT examinations in poly-trauma cases. The data revealed differences in radiation doses between the two sexes. The range of organ doses ranged from 1.76 mGy to 37.69 mGy for females and from 1.26 mGy to 32.97 mGy for males, with the thyroid receiving the highest dose and muscle receiving the lowest dose in both sexes. For the majority of organs, females received higher organ radiation doses than males did. The thyroid, kidney, lens, spleen, and brain were among the organs with the most significant dose differences. In females, the thyroid received a dose of 37.69 mGy, whereas in males, the dose was 32.97 mGy. Similarly, the kidney dose was 29.39 mGy in females and 22.59 mGy in males. The lens dose was 28.1 mGy in females and 25.72 mGy in males, whereas the spleen dose was 26.88 mGy in females and 21.99 mGy in males. The brain dose was 24.75 mGy in females and 19.92 mGy in males.
There were a few exceptions to the general trend of higher doses in females. The breast and heart wall doses were slightly higher in males than in females. The breast radiation dose was 22.26 mGy in males and 20.63 mGy in females, whereas the heart wall radiation dose was 21.99 mGy in males and 23.38 mGy in females. The radiation dose for the prostate in males was 14.72 mGy, whereas for the uterus in females, it was 13.94 mGy. The dose for testes in males was 6.41 mGy, and for ovaries in females, it was 17.34 mGy.
The results presented in Table 3 elucidate the LAR of cancer incidence and mortality, distinguishing between male and female populations across various cancer sites. The cumulative data for "All cancers" indicate a higher overall incidence and mortality rate for females (707 per 100,000 for incidence and 409 per 100,000 for mortality) than for males (609 per 100,000 for incidence and 324 per 100,000 for mortality). Considering both genders together, the overall LAR for all cancers stands at 658 cases per 100,000 individuals for incidence and 366 cases per 100,000 individuals for mortality.
Mean values ± SD, ranges and 50th (25th–75th) percentile of DLP, CTDIvol for WBCT examinations.
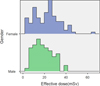 |
Fig. 1 Effective dose distribution of CT scans of the WB for trauma patients. |
 |
Fig. 2 Radiation organ doses of the WBCT scan for trauma patients. |
Lifetime attributable risk of cancer incidence and mortality.
4 Discussion
The assessment of radiation dose and associated cancer risk from WBCT examinations in poly-trauma patients is a critical area of investigation. Trauma patients undergo multiple CT scans as part of their diagnostic and treatment protocols, potentially exposing them to significant ionizing radiation (Godt et al., 2021; Hijji et al., 2023). This cumulative radiation exposure raises concerns about the long-term risk of radiation-induced cancers, necessitating a regular evaluation of effective doses and organ-specific radiation burdens.
The typical values are represented by the mean of the proposed reference level based on the 75th percentile and the achievable dose based on the 50th percentile. The most common value in the sample is used to determine the mode, which is used as an indicator of typical practice (Huber-Wagner et al., 2018). In the present study, the mean CTDIvol was 16.03 mGy, with a median of 15.9 mGy, and the 75th percentile was 21.13 mGy. The DLP mean was 1063.21 mGy · cm, with a median of 1043 mGy · cm, and the 75th percentile was 1456.5 mGy · cm. A similar study reported that the average CTDIvol was 59.2 mGy, with a median of 59.2 mGy, and a 75th percentile of 62 mGy. The DLP had a mean of 2774.4 mGy · cm, a median of 2762.6 mGy · cm, and a 75th percentile of 2873.4 mGy · cm (Abuzaid et al., 2022). The current study’s reported values for CTDIvol and DLP are lower than those of Abuzaid et al. The overall mean effective dose for all trauma patients who underwent a WBCT scan was 20.81 ± 10.78 mSv. Published data on WBCT suggest that average radiation doses vary from 10 to 31.8 mSv (Brenner et al., 2004; Davies et al., 2016; Sato et al., 2017; Harrieder et al., 2012; Sierink et al., 2016). Another previous study reported higher effective doses at 34.5 mSv (Abuzaid et al., 2022) and 29.5 mSv (Gordic et al., 2015), and another study reported a higher ED at 76 mSv (Asha et al., 2012). The mean effective dose (20.81 ± 10.78 mSv) in the current study is within the range reported by several previous studies but lower than those reported by Abuzaid et al., Gordic et al., and Asha et al.
The results of this study demonstrated differences in the radiation doses received by various organs between female and male patients who underwent WBCT examinations among poly-trauma patients. The organ doses from WBCT ranged from 1.76 to 37.69 mGy and from 1.26 to 32.79 mGy for females and males, respectively. A similar previous study reported that the organ doses from WBCT ranged from 10.2 to 63.7 mGy (Abuzaid et al., 2022). Although females in our sample had a slightly higher mean BMI (29.5±6.1kg/m2) than males (27.8±5.2kg/m2), BMI alone does not explain the observed dose distribution differences. These differences in organ doses may result from anatomical and compositional variations between sexes, scanner settings, or protocol adjustments. Additionally, the location of certain radiosensitive organs in females (e.g., breasts) often contributes to higher absorbed doses compared to males.
Patients with multiple traumatic injuries, who are often younger, face an elevated lifetime risk of radiation-induced cancer from CT imaging. Although precise individual risk remains uncertain, estimates suggest it is very low at doses under 0.2mSv (<1 in 100,000) but rises with higher exposures (ARPANSA, 2005). For example, Brenner et al. estimated that a 45-year-old adult undergoing a single WBCT scan at 10–20mSv faces a lifetime cancer mortality risk of approximately 0.08% (1 in 1,250) (Brenner et al., 2004). In our study, the estimated LAR of cancer incidence was 707 cases per 100,000 for females and 609 per 100,000 for males, with corresponding mortality risks of 409 cases per 100,000 and 324 per 100,000. While these risks are low in absolute terms, they are not negligible, especially in younger patients. Importantly, the justification principle remains critical: in emergency departments, high-dose WBCT may be warranted when rapid, comprehensive diagnosis is needed to guide life-saving treatment. Clinical decisions must therefore balance potential radiation risks with the clear, immediate benefits of timely and accurate assessment in trauma care.
Optimizing the radiation dose from WBCT in trauma patients with multiple injuries is crucial to minimize potential risks while maintaining diagnostic accuracy. Several dose reduction strategies can be employed, such as using iterative reconstruction algorithms, lowering the tube voltage and current, and utilizing automatic exposure control systems (Purcell et al., 2020; Mulas et al., 2022). Advances in CT technology have enabled significant dose reductions in WBCT protocols without compromising image quality (Elmokadem et al., 2019; Simma et al., 2022). A study demonstrated that using a low-dose WBCT protocol with iterative reconstruction resulted in a 40% reduction in radiation dose compared with a standard protocol while maintaining comparable diagnostic accuracy (Elmokadem et al., 2019). Additionally, protocol optimization based on clinical indications and patient-specific factors can further reduce radiation exposure. At our emergency department, targeted scanning of critical body regions such as the head and cervical spine, followed by a single-phase acquisition of the thorax, abdomen, and pelvis, is routinely practiced to avoid unnecessary radiation exposure. Careful patient positioning, limiting scan ranges, and minimizing repeat acquisitions are integral components of our established procedures. Ultimately, our goal aligns with the ALARA (as low as reasonably achievable) principle, carefully balancing timely and accurate diagnoses with minimized radiation doses, tailored to the specific clinical scenarios encountered in trauma care (Purcell et al., 2020; Mulas et al., 2022).
This study has several limitations. First, there are differences between the Saudi population’s baseline cancer incidence levels and mortality rates and those listed in the BEIR VII study (NRC, 2006). Second, the LAR of cancer occurrence from X-rays ranged from 80−140 kVp, possibly distinct from that of high-energy gamma rays, for which the BEIR VII database represents a majority of cases on the basis of these high-energy rays (Kim et al., 2010).
5 Conclusion
The findings of this study highlight the significant radiation exposure associated with WBCT in trauma patients, emphasizing the need for careful consideration of its use in clinical practice. Our results indicate a considerable effective dose received by patients, with a mean value of 20.81 ± 10.78 mSv and a lifetime cancer risk of 0.65% for incidence and 0.36% for mortality. WBCT scanning carries a substantial risk of developing cancer due to this significant radiation exposure. Therefore, the use of WBCT should be clinically justified, and measures must be taken to reduce the radiation dose.
Acknowledgments
The authors gratefully acknowledge the funding of the Research, Development, and Innovation Authority (RDIA) - Kingdom of Saudi Arabia - with grant number (12899-jazzan-2023-JZU-R-2-1-HW).
Funding
This article is derived from a research grant funded by the Research, Development, and Innovation Authority (RDIA) - Kingdom of Saudi Arabia - with grant number (12899-jazzan-2023-JZU-R-2-1-HW).
Conflicts of interest
The authors declares that he has no conflicts of interest in relation to this article.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics approval
The study adhered to ethical guidelines and complied with the principles of the Declaration of Helsinki.
Informed consent
The need for informed consent was waived by Jazan University’s institutional review board due to the retrospective nature of the data.
References
- Abuzaid MM, Tekin HO, Elshami W, Almisned G, Ene A, Zakaly HMH. 2022. Radiation dose assessment in multiple injured patients using whole-body computed tomography. J Radiat Res Appl Sci 15: 100465. [Google Scholar]
- ARPANSA. 2005. Code of Practice for the Exposure of Humans to Ionizing Radiation for Research Purposes. Radiation Protection Series Publication No. 8. Australian Radiation Protection and Nuclear Safety AgencyPlace. Published [Google Scholar]
- Asha S, Curtis KA, Grant N, Taylor C, Lo S, Smart R, Compagnoni K. 2012. Comparison of radiation exposure of trauma patients from diagnostic radiology procedures before and after the introduction of a panscan protocol. Emerg Med Australasia 24: 43–51. [Google Scholar]
- Brenner DJ, Elliston CD. 2004. Estimated radiation risks potentially associated with full-body CT screening. Radiology 232: 735–738. [Google Scholar]
- Davies RM, Scrimshire AB, Sweetman L, Anderton MJ, Holt EM. 2016. A decision tool for whole-body CT in major trauma that safely reduces unnecessary scanning and associated radiation risks: an initial exploratory analysis. Injury 47: 43–49. [Google Scholar]
- Elmokadem AH, Ibrahim EA, Gouda WA, Khalek Abdel Razek AA. 2019. Whole-body computed tomography using low-dose biphasic injection protocol with adaptive statistical iterative reconstruction v: assessment of dose reduction and image quality in trauma patients. J Comput Assist Tomogr 43: 870–876. [Google Scholar]
- Godt JC, Johansen CK, Martinsen ACT, Schulz A, Brogger HM, Jensen K, Stray-Pedersen A, Dormagen JB. 2021. Iterative reconstruction improves image quality and reduces radiation dose in trauma protocols: a human cadaver study. Acta Radiol Open 10: 20584601211055389. [Google Scholar]
- Gordic S, Alkadhi H, Hodel S, Simmen HP, Brueesch M, Frauenfelder T, Wanner G, Sprengel K. 2015. Whole-body CT-based imaging algorithm for multiple trauma patients: radiation dose and time to diagnosis. Br J Radiol 88: 20140616. [Google Scholar]
- Harrieder A, Geyer LL, Korner M, Deak Z, Wirth S, Reiser M, Linsenmaier U. 2012. Evaluation of radiation dose in 64-row whole-body CT of multiple injured patients compared to 4-row CT. Rofo 184: 443–449. [Google Scholar]
- Hijji FY, Schneider AD, Thomas MD, Lyons JG, Bohl DD, Jerele JL, Prayson MJ. 2023. Knowledge of radiation exposure associated with common trauma imaging modalities among orthopaedic surgeons, emergency medicine physicians, and general surgeons in the United States. World J Emerg Med 14: 294–301. [Google Scholar]
- Huber-Wagner S, Kanz KG, Hanschen M, van Griensven M, Biberthaler P, Lefering R. 2018. Whole-body computed tomography in severely injured patients. Curr Opin Crit Care 24: 55–61. [Google Scholar]
- Huber-Wagner S, Lefering R, Qvick LM, Korner M, Kay MV, Pfeifer KJ, Reiser M, Mutschler W, Kanz KG, Working Group on Polytrauma of the German Trauma S. 2009. Effect of whole-body CT during trauma resuscitation on survival: a retrospective, multicentre study. Lancet 373: 1455–1461. [CrossRef] [PubMed] [Google Scholar]
- ICRP. 2007. The 2007 recommendations of the international commission on radiological protection. ICRP publication 103. Ann. ICRP 2007. [Google Scholar]
- Jiang L, Ma Y, Jiang S, Ye L, Zheng Z, Xu Y, Zhang M. 2014. Comparison of whole-body computed tomography vs selective radiological imaging on outcomes in major trauma patients: a meta-analysis. Scand J Trauma Resusc Emerg Med 22: 54. [Google Scholar]
- Kim S, Yoshizumi TT, Frush DP, Toncheva G, Yin FF. 2010. Radiation dose from cone beam CT in a pediatric phantom: risk estimation of cancer incidence. Am J Roentgenol 194: 186–190. [Google Scholar]
- Lee C, Kim KP, Bolch WE, Moroz BE, Folio L. 2015. NCICT: a computational solution to estimate organ doses for pediatric and adult patients undergoing CT scans. J Radiol Prot 35: 891–909. [Google Scholar]
- Moorin RE, Gibson DA, Forsyth RK, Fox R. 2014. Demonstration of the effect of generic anatomical divisions versus clinical protocols on computed tomography dose estimates and risk burden. PLoS One 9: e97691. [Google Scholar]
- Mulas V, Catalano L, Geatti V, Alinari B, Ragusa F, Golfieri R, Orlandi PE, Imbriani M. 2022. Major trauma with only dynamic criteria: is the routine use of whole-body CT as a first level examination justified? Radiol Med 127: 65–71. [Google Scholar]
- NRC. (2006). Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2. Washington, DC: The National Academies Press. https://doi.org/10.17226/11340 [Google Scholar]
- Purcell LN, Charles A. 2020. Low-dose whole-body computed tomography and radiation exposure in patients with trauma-trust, but verify. JAMA Surg 155: 232. [Google Scholar]
- Sato T, Saito Y, Saito N, Ooba M. 2017. Multicenter investigation of the effective dose for whole-body CT scanning. Nihon Hoshasen Gijutsu Gakkai Zasshi 73: 258–266. [Google Scholar]
- Sierink JC, Treskes K, Edwards MJ, Beuker BJ, den Hartog D, Hohmann J, Dijkgraaf MG, Luitse JS, Beenen LF, Hollmann MW, Goslings JC, Group R.-S. 2016. Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial. Lancet 388: 673–683. [Google Scholar]
- Simma L, Fornaro J, Stahr N, Lehner M, Roos JE, Lima TVM. 2022. Optimising whole body computed tomography doses for paediatric trauma patients: a Swiss retrospective analysis. J Radiol Prot 42. [Google Scholar]
- Weber L, Hansson M, Geijer M. 2023. Computed tomography with adjusted dose for body mass index may be superior to whole-body radiography especially in elderly patients with multiple myeloma. Acta Radiol 64: 1896–1903. [Google Scholar]
- Wen JC, Sai V, Straatsma BR, McCannel TA. 2013. Radiation-related cancer risk associated with surveillance imaging for metastasis from choroidal melanoma. JAMA Ophthalmol 131: 56–61. [Google Scholar]
- Zensen S, Bos D, Opitz M, Haubold J, Forsting M, Guberina N, Wetter A. 2022. Radiation exposure and establishment of diagnostic reference levels of whole-body low-dose CT for the assessment of multiple myeloma with second- and third-generation dual-source CT. Acta Radiol 63: 527–535. [Google Scholar]
Cite this article as: Shubayr N. 2026. Assessment of radiation risk associated with whole-body computed tomography at the emergency department. Radioprotection 61(1): 62–67. https://doi.org/10.1051/radiopro/2025023
All Tables
Mean values ± SD, ranges and 50th (25th–75th) percentile of DLP, CTDIvol for WBCT examinations.
All Figures
|
Fig. 1 Effective dose distribution of CT scans of the WB for trauma patients. |
| In the text | |
|
Fig. 2 Radiation organ doses of the WBCT scan for trauma patients. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.