")
")
| Issue |
Radioprotection
Volume 60, Number 2, Avril-Juin 2025
|
|
|---|---|---|
| Page(s) | 168 - 175 | |
| DOI | https://doi.org/10.1051/radiopro/2024044 | |
| Published online | 13 June 2025 | |
Article
Evaluating the knowledge of radiation exposure parameters among CT technologists in Saudi Arabia: A survey-based study on adherence to ALARA principles and dose optimization
Radiological Sciences Department, College of Applied Medical Sciences, King Saud University, P.O. Box 145111, Riyadh, 4545, Saudi Arabia
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
15
July
2024
Accepted:
16
September
2024
Abstract
Computed tomography is a crucial tool in modern healthcare, offering non-invasive imaging for diagnosis and monitoring. However, its widespread use raises concerns about radiation exposure. Adhering to the ALARA principle is vital to minimize risks while maintaining diagnostic quality. This study evaluates the knowledge of CT technologists in Saudi Arabia regarding radiation exposure parameters. A questionnaire-based survey was conducted, covering demographics, perceptions, and understanding of CT parameters. Statistical analysis revealed gaps in knowledge, particularly regarding dose optimization strategies and diagnostic reference levels. While most participants recognized the importance of adjusting parameters based on patient characteristics and clinical indications, deficiencies were observed in understanding specific parameters’ effects on dose and image quality. Furthermore, a notable proportion of participants were unfamiliar with DRLs, indicating a need for improved education in this area. The study emphasizes the importance of interdisciplinary collaboration between radiologists, physicists, and technologists in protocol development and optimization.
Key words: Knowledge / radiation dose / risk / CT scan / Saudi Arabia
© Y. Alashban and S.A. Alghamdi, Published by EDP Sciences 2025
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
1 Introduction
Computed tomography (CT) has transformed modern healthcare by enabling non-invasive visualization of internal bodily structures, facilitating swift disease diagnosis and monitoring. This advancement has significantly enhanced patient care standards, establishing CT as the preferred imaging modality for various medical purposes. Nonetheless, CT is associated with some of the highest radiation doses in diagnostic radiology and, given its expanding global usage (UNSCEAR, 2008), it is becoming the primary contributor to the population’s radiation exposure from medical procedures (NCRP, 2009). Concerns are growing regarding the potential harm that CT may pose to both populations (Brenner and Hall, 2007; Pearce et al., 2012) and individuals (Zarembo, 2009; Bogdanich, 2010), particularly when used inappropriately due to its carcinogenic potential (Jameson, 2005).
For CT examinations to be justifiable, they must adhere to the ’As Low As Reasonably Achievable’ (ALARA) principle, aiming to minimize patient radiation exposure to ensure that the benefits always outweigh the potential risks (ICRP, 2007). Achieving this optimization requires a deep understanding of the various factors influencing radiation output in CT, such as peak kilovoltage (kVp), tube current–time product (mAs), pitch, slice thickness, and more. CT image quality is directly linked to the amount of radiation used, emphasizing the need for an appropriate balance: enough radiation for a diagnostic yield while avoiding excessive radiation that increases patient risk. Users have a wide array of CT parameter combinations to choose from, producing various trade-offs between image quality and dose (Amis et al., 2007), some of which may be manufacturer-specific. Default settings and manufacturer-recommended protocols often prioritize image quality over patient dose. To achieve optimization, users must tailor CT parameters based on the clinical indication, the scanned region, and the patient’s size, recognizing that not all examinations require the highest level of detail. However, this necessitates a specialized understanding of CT and a substantial time commitment, particularly in busy healthcare settings.
Research reveals significant variations in radiation dose between facilities and across countries, even for patients of similar size (Foley et al., 2012), attributed to differences in CT equipment and local scanning protocols. Such discrepancies may also indicate a lack of awareness or manipulation of parameters, especially on an individual basis. Some studies have found that up to 25% of radiologists, who play a crucial role in interpreting CT scan images to diagnose medical conditions and guide patient treatment, are unaware of the specific CT parameters used in routine examinations (Hollingsworth et al., 2003). As CT technology continues to advance, users may face challenges in becoming familiar with the features of their specific system, particularly when operating multiple scanner models from different manufacturers. The recent introduction of automated tube current modulation (ATCM) has greatly aided users in tailoring patient doses (Rizzo et al., 2006), and its success has led to the introduction of further automated systems (Yu et al., 2010). However, a comprehensive understanding of such software is essential to ensure its proper operation and use (Gudjonsdottir et al., 2009; Matsubara et al., 2009) . This study aims to assess the current knowledge of a selected group of radiologists and technologists and identify potential areas requiring improvement.
2 Methods
The study complies with the Declaration of Helsinki, adhering to ethical standards and receiving approval from the Institutional Review Board at Prince Sattam bin Abdulaziz University (Ref. SCBR-281/2024). Informed consent was obtained from all participants prior to their involvement in the study.
This cross-sectional study, conducted in January and February 2024, utilized an online questionnaire distributed across various hospitals in Saudi Arabia using CT scanners. The questionnaire was sent to the CT supervisors of each hospital via an online request, which detailed the study’s objectives and benefits and requested further distribution to CT technologists, who are responsible for operating the CT machines, selecting appropriate imaging parameters, and ensuring patient safety during the scan . A total of 86 hospitals were approached to participate in the study.
The survey questionnaire, adopted from source (Foley et al., 2013) included 47 questions divided into two sections. Section A collected basic demographic data and gathered opinions on CT radiation doses, while Section B contained questions about specific CT scan protocols, parameters, and diagnostic reference levels. The format predominantly featured true/false and multiple-choice questions, with questions based on a five-point Likert scale. Responses to the questions about specific CT parameters were scored, with correct answers receiving a score of 1 and incorrect receiving a score of 0. Each survey included a cover letter that explained the survey’s purpose and provided instructions for completion, ensuring complete respondent anonymity.
Statistical analysis was performed using SPSS version 27, with a P value of less than 0.05 indicating statistical significance. Descriptive statistics were used to evaluate the questionnaire items. The choice between the Mann-Whitney U test and independent samples t-tests depended on the results of the Kolmogorov-Smirnov normality test. For open-ended questions, thematic analysis was conducted to identify recurring themes and patterns.
3 Results
A total of 328 technologists responded to the questionnaire (response rate = 89%) to evaluate their knowledge regarding radiation exposure parameters. In the present investigation, our study cohort exhibited a predominance of male participants (n = 224, 68.3%) and a majority of technologists employed within public sector hospitals (n = 264, 60.5%). A substantial proportion of respondents (n = 272, 82.9%) conveyed that radiologists bear the primary responsibility for establishing protocols for routine CT scans, while (n = 8, 2.4%) of responders highlighted that physicists, who are responsible for ensuring the optimal performance of the CT scanner, managing radiation dose, and maintaining image quality through equipment calibration, quality control, and protocol optimization, are the ones responsible for establishing routine CT scan protocols. It was observed that 228 participants (69.5%) affirmed having modified CT protocols within the preceding 2 yr, and 288 participants (87.8%) expressed a belief in the potential advantages of further education in this domain (see Tab. 1). Application specialists in CT imaging provide training and support to technologists and radiologists, helping them effectively use the CT equipment and software, optimize imaging protocols, and implement new technologies.
The data reveals that 62.19% (n = 204) of the respondents demonstrated confidence in their capacity to adjust CT parameters accurately, taking into consideration both image quality and radiation dose, whereas 14.63% (n = 48) reported a poor or very poor level of confidence. (Fig. 1). Routine CT scanning parameters such as kVp, mAs, slice thickness, pitch, reconstruction algorithms, among others, were deemed adjustable based on patient size (98.8%), anatomical region (89.0%), study indication (79.3%), and patient age (82.9%). It was noted that 90.2% of participants concurred that Automatic Tube Current Modulation (ATCM) results in an average reduction in patient dose.
Additionally, most participants (n = 228, 69.5%) did not consider it necessary to employ the same noise setting for the non-contrast phase of an abdominal scan as for the contrast phase. Concerning the question regarding the reduction of kVp from 120 to 100 for angiographic CT procedures while keeping all other parameters constant, 91.5% (n = 300) of the participants concurred that it leads to a decrease in radiation dose, with 68.3% (n = 224) agreeing on an increase in image noise and 31.7% (n = 104) dissenting. The majority of respondents (n = 256, 78%) correctly recognized that higher table speeds, which enhance slice sensitivity profiles, result in a diminished z-axis resolution (Tab. 2).
In the context of construction parameters, it was revealed that 62.19% (n = 204) of participants considered it inaccurate that a smoothing reconstruction kernel enhances noise visualization. Furthermore, 85.36% (n = 280) concurred that a wide window setting diminishes image contrast and visual perception of noise (Fig. 2). Our investigation found that 54.9% of participants reported an increase in CTDI values of 38% when increasing the peak beam energy (kVp) from 120 to 140 kVp, with only 2.4% asserting an 89% increase in CRDI (see Fig. 3). The study identified a substantial proportion of participants who strongly believed that multiple factors influence image noise, with 304 participants attributing this to kVp and 292 to mA. Moreover, 172 participants identified Window width and window level as contributing factors (Fig. 4).
Notably, 41.5% (n = 136) of the subjects accurately identified the Diagnostic Reference Level (DRL) for the Adult Head, as recommended by national standards to be 50 mGy CTDIvol, while only 24.07% (n = 52) correctly reported the appropriate dose for the adult abdomen and pelvis. Additionally, 52.94% (n = 108) of the participants accurately selected the suitable dosage of 12 mGy for the adult chest, and 36.6% (n = 64) accurately indicated the appropriate dosage for the pediatric head (Tab. 3). In Saudi Arabia, the Saudi Food and Drug Authority (SFDA) is the reference for the national DRL and provides guidelines and standards for medical imaging and radiation safety. According to the most recent national DRL report published by the SFDA in 2022, the DRL for adult CT scans of the head, abdomen and pelvis, and chest are approximately 55 mGy, 14 mGy CTDIvol, and 12 mGy, respectively (SFDA, 2022).
Participants response regarding demographic and CT protocols.
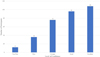 |
Fig. 1 Confidence of participants to change the CT parameters correctly, considering image quality and radiation dose. |
Participants response regarding different aspects.
 |
Fig. 2 Response of the participants towards different reconstruction parameters. |
 |
Fig. 3 Relationship of CTDI values of when increasing the peak beam energy. |
 |
Fig. 4 Image noise is influenced by which of the following factors. |
Response of the participant regarding the national recommended DRL (CTDIvol) for different categories.
4 Discussion
The findings of this study offer valuable insights into the knowledge and comprehension of CT technologists in Saudi Arabia pertaining to CT exposure parameters. The results underscore distinct areas that warrant further educational and training interventions to improve the understanding and application of these criteria.
A significant proportion of CT technologists demonstrated a commendable recognition of patient size as a pivotal variable that should influence the selection of parameters for routine CT scanning. This recognition is of paramount importance, as the judicious adjustment of settings according to patient size plays a critical role in optimizing both radiation dose and image quality (Dougeni et al., 2012). A substantial proportion of the surveyed participants (82.9%, n = 272) expressed their belief that radiologists hold the primary responsibility for establishing protocols for routine CT scans. This finding suggests the need for interdisciplinary communication and collaboration, particularly between radiologists and CT technologists, to ensure a coherent and well-informed approach to protocol development. Conversely, 2.4% of the participants (n = 8) highlighted that physicists are the ones responsible for establishing routine CT scan protocols. This finding may indicate a potential gap in the involvement of physicists in CT protocol development and optimization, which warrants further investigation.
Moreover, 69.5% of the participants (n = 228) acknowledged having modified CT protocols within the past 2 yr. This suggests an active engagement in protocol adjustments, reflecting a dynamic environment where technologists are willing to adapt to evolving best practices and technological advancements. Additionally, a substantial 87.8% of the participants (n = 288) recognized the potential advantages of further education in the domain of CT technology. This finding underscores the importance of ongoing professional development and the willingness of CT technologists to enhance their knowledge and skills in this rapidly evolving field.
A noteworthy majority of the participants (69.5%, n = 228) did not perceive the necessity of applying the same noise setting for the non-contrast phase of an abdominal CT scan as for the contrast-enhanced phase. This recognition is of paramount importance as it reflects an understanding that noise levels can be adjusted to suit the specific requirements of each phase, which can lead to improved image quality and diagnostic accuracy.
When participants asked about the potential effect of reducing the kilovoltage peak (kVp) from 120 to 100 for angiographic CT procedures while keeping all other parameters constant, a substantial 91.5% of the participants (n = 300) concurred that such a reduction results in a decrease in radiation dose. Moreover, 68.3% of participants (n = 224) agreed that this change would lead to an increase in image noise, while 31.7% (n = 104) dissented. These findings highlight a general understanding among the technologists that reducing kVp can effectively lower radiation exposure, but there is a divergence of opinion regarding the impact on image noise. This indicates the need for clear guidelines and training in this area to reconcile and optimize the balance between dose reduction and image quality maintenance. Additionally, the study identified that the majority of respondents (78%, n = 256) correctly recognized the influence of higher table speeds on slice sensitivity profiles and the resulting decrease in z-axis resolution. This finding underscores the awareness of the trade-offs associated with faster table speeds, where improved coverage and reduced scan time must be weighed against potential reductions in image sharpness and diagnostic precision.
Elevating the peak beam energy (kVp) from 120 to 140 kVp, as expounded in this investigation, induces a discernible rise in the CTDI values. As indicated in a prior study, augmenting the peak kilovoltage amplifies the radiation dose imparted by the X-ray beam, under the condition of keeping all other pertinent parameters constant (Goldman, 2007). In the realm of CT imaging, the manifestation of image noise is subject to the influence of multiple contributing factors. The participants in this study attributed paramount significance to several variables, notably including mA, kVp, helical pitch, and slice thickness, as pivotal determinants of image noise. This finding aligns with the conclusions drawn in a prior investigation by Juluru et al. (2013) where the study affirmed that tube current, tube rotation speed, peak voltage, pitch, and collimation hold substantial sway over the radiation exposure encountered in the course of a CT scan. In accordance with the findings of this investigation, a mere 41.5% of the respondents provided the correct (DRL) for the adult head, while 15.9% accurately identified the DRL for the adult abdomen and pelvis, 32.9% for the adult chest, and 19.5% for the pediatric head. These outcomes bear a noteworthy resemblance to those reported in a separate study, wherein 45.8% of the respondents demonstrated an aptitude for accurately comprehending the underlying principles of DRLs (Abdulkadir et al., 2021). The present study has revealed certain deficiencies in the knowledge of DRLs among the technologists, particularly in terms of executing local dose surveys for DRLs and the principles of optimization. To address these gaps, a heightened emphasis should be placed on incorporating educational components related to dose optimization and institutional-specific dose assessments within the continued training and professional development of CT technologists.
The results underscore the imperative for supplementary training and pedagogical interventions to enhance the proficiency of CT technologists in matters pertaining to exposure parameters, strategies for noise mitigation, and techniques for dose optimization. Through the augmentation of technologists’ expertise and competencies in these domains, there exists the prospect of more effective execution of optimal imaging protocols, reduced radiation exposure, and heightened levels of patient safety (Kazemi et al., 2023). The results demonstrate the significance of maintaining dosage optimization efforts. It is essential to compare the radiation dosage limits for various CT examinations to the nationally accepted DRLs. In the future, it will be necessary to revise these DRLs to ensure they remain current with technological advances, imaging standards, and best practices. The objective should be to obtain diagnostic imaging with minimal radiation exposure without sacrificing image quality (Vañó et al., 2017). Future advancements in CT technology should strive to improve image quality and reduce radiation doses simultaneously. Innovations in reconstruction algorithms, state-of-the-art noise reduction techniques, and cutting-edge imaging techniques have the potential to bring about significant enhancements. In addition, developing and implementing dose reduction technologies, such as iterative reconstruction algorithms and automated exposure control systems, can substantially contribute to reducing radiation doses without sacrificing image quality (Yu et al., 2009; McLeavy et al., 2021).
This study identifies some knowledge deficits among CT technologists, particularly regarding parameters influencing image noise, although overall awareness of dose optimization and adherence to ALARA principles is strong. More than 50% of respondents answered correctly in most areas, with some reaching up to 80%, though gaps remain in understanding specific technical aspects such as DRLs. These findings align with those of (Shubayr et al., 2024), who assessed medical radiological technologists (MRTs) and found strong knowledge in radiation safety culture, though MRTs encompass a broader range of imaging professionals than CT technologists. Similarly, a study conducted by Alomairy et al. (2024) observed knowledge gaps among nurses in pediatric intensive care units (PICUs) regarding radiation protection, though nurses are less involved in adjusting imaging parameters than CT technologists. The differences in knowledge across these populations highlight the need for targeted, role-specific educational interventions. For CT technologists, focused training on DRLs and patient-specific dose adjustments could help close knowledge gaps and further enhance radiation safety practices.
This research has limitations that must be considered. First, only a small number of technologists in Saudi Arabia were given the questionnaire, so the sample size may not be representative of the entire profession. Future studies should strive for a larger and more representative sample in order to gain a more comprehensive understanding of knowledge gaps among CT technologists across the country.
In addition, this research relied on self-reported knowledge, which introduces the possibility of exaggerated or biased responses. Recognizing the potential influence of participants’ subjective perceptions on results is essential.
5 Conclusion
This study identifies some knowledge deficits among CT technologists, particularly in understanding the parameters that influence image noise. Nevertheless, the overall findings indicate that CT technologists possess a solid grasp of dose optimization principles and are proficient in adjusting key parameters to ensure patient safety. While certain areas require further attention, targeted educational interventions aimed at improving knowledge of DRLs and patient-specific dose adjustments will enhance radiation safety practices and optimize patient care.
There are some discrepancies between the population studied and the specialties concerning knowledge and attitudes regarding radiation protection in general, and the radiation protection of patients in particular, as highlighted in the study. The findings emphasize the importance of instituting ongoing education and training programs for CT technologists to enhance their skills and knowledge. Specifically, CT technologists would benefit from a more comprehensive understanding of exposure parameters, noise reduction techniques, and dose optimization strategies. Adhering to nationally approved DRLs is essential to ensure that patients undergoing CT exams receive safe radiation doses. Future success requires continued efforts to optimize dosage, improve technologist training, and leverage technological advancements. These initiatives should prioritize the reduction of radiation doses without compromising image quality or patient safety
Funding
The authors would like to extend their sincere appreciation to the Researchers supporting program for funding this work under Researchers Supporting Project number (RSPD2024R780), King Saud University, Riyadh, Saudi Arabia.
Conflicts of interest
The authors declare to have no conflicts of interest in regards to this article.
Author contribution statement
Yazeed Alashban contributed to the study’s conceptualization, methodology design, data analysis, drafting the manuscript, and interpreting the results.
Sami A. Alghamdi contributed to data collection, statistical analysis, manuscript revision, interpretation of the findings, and provided critical insights into the study’s implications.
Ethics approval
The study complies with the Declaration of Helsinki, adhering to ethical standards and receiving approval from the Institutional Review Board at Prince Sattam bin Abdulaziz University (Ref. SCBR-281/2024).
Informed consent
Informed consent was obtained from all participants prior to their involvement in the study.
References
- Abdulkadir MK, Piersson AD, Musa GM, Audu SA, Abubakar A, Muftaudeen B, Umana JE. 2021. Assessment of diagnostic reference levels awareness and knowledge amongst ct radiographers. Egypt J Radiol Nucl Med 52: 1–8. https://doi.org/10.1186/s43055-021-00444-x. [CrossRef] [Google Scholar]
- Alomairy NA. 2024. Evaluating the knowledge and attitudes towards radiation protection in portable radiological examinations among nurses in pediatric intensive care units. Radioprotection 59: 36–41. https://doi.org/10.1051/radiopro/2023044. [CrossRef] [EDP Sciences] [Google Scholar]
- Amis ES Jr., Butler PF, Applegate KE, Birnbaum SB, Brateman LF, Hevezi JM, Mettler FA, Morin RL, Pentecost MJ, Smith GG, Strauss KJ, Zeman RK. 2007. American college of radiology white paper on radiation dose in medicine. J Am Coll Radiol 4: 272–284. https://doi.org/10.1016/j.jacr.2007.03.002. [Google Scholar]
- Bogdanich W. 2010. After stroke scans, patients face serious health risks. The New York Times 31: 1–9. http://www.nytimes.com/2010/08/01/health/01radiation.html? [Google Scholar]
- Brenner DJ, Hall EJ. 2007. Computed tomography-an increasing source of radiation exposure. N Engl J Med 357: 2277–2284. https://doi.org/10.1056/NEJMra072149. [CrossRef] [PubMed] [Google Scholar]
- Dougeni E, Faulkner K, Panayiotakis G. 2012. A review of patient dose and optimisation methods in adult and paediatric ct scanning. Eur J Radiol 81: 665–683. https://doi.org/10.1016/j.ejrad.2011.03.006. [Google Scholar]
- Foley SJ, Evanoff MG, Rainford LA. 2013. A questionnaire survey reviewing radiologists’ and clinical specialist radiographers’ knowledge of ct exposure parameters. Insights Imaging 4: 637–646. https://doi.org/10.1007/s13244-013-0277-2. [CrossRef] [PubMed] [Google Scholar]
- Foley SJ, McEntee MF, Rainford LA. 2012. Establishment of ct diagnostic reference levels in ireland. Br J Radiol 85: 1390–1397. https://doi.org/10.1259/bjr/25026136. [CrossRef] [PubMed] [Google Scholar]
- Goldman LW. 2007. Principles of ct: radiation dose and image quality. J Nucl Med Tec 35: 213–225. https://doi.org/10.2967/jnmt.106.037846. [CrossRef] [PubMed] [Google Scholar]
- Gudjonsdottir J, Svensson JR, Campling S, Brennan PC, Jonsdottir B. 2009. Efficient use of automatic exposure control systems in computed tomography requires correct patient positioning. Acta Radiol 50: 1035–1041. https://doi.org/10.3109/02841850903232850. [CrossRef] [PubMed] [Google Scholar]
- Hollingsworth C, Frush DP, Cross M, Lucaya J. 2003. Helical ct of the body: a survey of techniques used for pediatric patients. Am J Roentgenol 180: 401–406. https://doi.org/10.2214/ajr.180.2.1800401. [CrossRef] [PubMed] [Google Scholar]
- ICRP. International commission on radiation protection. 2007. Managing patient dose in multi-detector computed tomography (mdct). Publication 102. Ann ICRP 37: 1–85. [Google Scholar]
- Jameson C. 2005. Report on carcinogens—history and process. Chem Health Saf 12: 9–14. https://doi.org/10.1016/j.chs.2004.11.006. [CrossRef] [Google Scholar]
- Juluru K, Shih JC, Raj A, Comunale JP, Delaney H, Greenberg ED, Hermann C, Liu YB, Hoelscher A, Al-Khori N, Sanelli PC. 2013. Effects of increased image noise on image quality and quantitative interpretation in brain ct perfusion. AJNR 34: 1506–1512. https://doi.org/10.3174/ajnr.A3424. [CrossRef] [PubMed] [Google Scholar]
- Kazemi Z, Hajimiri K, Saghatchi F, Molazadeh M, Rezaeejam H. 2023. Assessment of the knowledge level of radiographers and ct technologists regarding computed tomography parameters in iran. Radiat Med Prot 4: 60–64. https://doi.org/10.1016/j.radmp.2022.11.005. [CrossRef] [Google Scholar]
- Matsubara K, Koshida K, Ichikawa K, Suzuki M, Takata T, Yamamoto T, Matsui O. 2009. Misoperation of ct automatic tube current modulation systems with inappropriate patient centering: phantom studies. Am J Roentgenol 192: 862–865. https://doi.org/10.2214/AJR.08.1550. [CrossRef] [PubMed] [Google Scholar]
- McLeavy CM, Chunara MH, Gravell RJ, Rauf A, Cushnie A, Staley Talbot C, Hawkins RM. 2021. The future of ct: deep learning reconstruction. Clin Radiol 76: 407–415. https://doi.org/10.1016/j.crad.2021.02.011. [CrossRef] [PubMed] [Google Scholar]
- NCRP. 2009. Ionizing radiation exposure of the population of the united states. [Google Scholar]
- Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, Kim KP, Howe NL, Ronckers CM, Rajaraman P, Sir Craft AW, Parker L, Berrington de Gonzalez A. 2012. Radiation exposure from ct scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet 380: 499–505. [CrossRef] [PubMed] [Google Scholar]
- Rizzo S, Kalra M, Schmidt B, Dalal T, Suess C, Flohr T, Blake M, Saini S. 2006. Comparison of angular and combined automatic tube current modulation techniques with constant tube current ct of the abdomen and pelvis. Am J Roentgenol 186: 673–679. https://doi.org/10.2214/AJR.04.1898. [CrossRef] [PubMed] [Google Scholar]
- Saudi Food and Drug Authority. 2022. National diagnostic reference levels. SFDA 2: 1–8. [Google Scholar]
- Shubayr N, Muawwadhah MD, Shami M, Jassas H, Tawhari R, Oraybi O, Madkhali A, Aldosari A, Alashban Y. 2024. Assessment of radiation safety culture among radiological technologists in medical imaging departments in Saudi Arabia. Radioprotection 59: 30–35. https://doi.org/10.1051/radiopro/2023042. [CrossRef] [EDP Sciences] [Google Scholar]
- UNSCEAR. 2008. Effects of ionizing radiation. Scientific Annexes E: 203–204. [Google Scholar]
- Vañó E, Miller D, Martin C, Rehani M, Kang K, Rosenstein M, Ortiz-López P, Mattsson S, Padovani R, Rogers A. 2017. ICRP publication 135: diagnostic reference levels in medical imaging. Annals ICRP 46: 1–144. [Google Scholar]
- Yu L, Li H, Fletcher JG, McCollough CH. 2010. Automatic selection of tube potential for radiation dose reduction in ct: a general strategy.Med Phys 37: 234–43. https://doi.org/10.1118/1.3263618. [CrossRef] [PubMed] [Google Scholar]
- Yu L, Liu X, Leng S, Kofler JM, Ramirez-Giraldo JC, Qu M, Christner J, Fletcher JG, McCollough CH. 2009. Radiation dose reduction in computed tomography: techniques and future perspective. Img Med 1: 65–84. https://doi.org/10.2214/ajr.07.3340. [Google Scholar]
- Zarembo A. 2009. Cedars-sinai investigated for significant radiation overdoses of 206 patients. Los Angeles Times. https://esciencenews.com/sources/la.times.science/2009/10/10/cedars.sinai.investigated.significant.radiation.overdoses.206.patients. [Google Scholar]
Cite this article as: Alashban Y, Alghamdi SA. 2025. Evaluating the knowledge of radiation exposure parameters among CT technologists in Saudi Arabia: A survey-based study on adherence to ALARA principles and dose optimization. Radioprotection 60(2): 168–175. https://doi.org/10.1051/radiopro/2024044
All Tables
Response of the participant regarding the national recommended DRL (CTDIvol) for different categories.
All Figures
|
Fig. 1 Confidence of participants to change the CT parameters correctly, considering image quality and radiation dose. |
| In the text | |
|
Fig. 2 Response of the participants towards different reconstruction parameters. |
| In the text | |
|
Fig. 3 Relationship of CTDI values of when increasing the peak beam energy. |
| In the text | |
|
Fig. 4 Image noise is influenced by which of the following factors. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.